A 58-year-old woman presented to her physician with a chief concern of mass of her anterior neck, of several years’ duration. She was also experiencing dysphagia and hoarseness. Review of her medical history revealed no medical conditions or medications. The patient had smoked cigarettes for many years. The mass was firm to palpation. It was centered in the thyroid gland and was fixed to underlying anatomic structures, per radiographic evaluation. At the time of presentation, the patient was euthyroid. A total thyroidectomy was performed, with suspicion for a malignant process.
Q1.
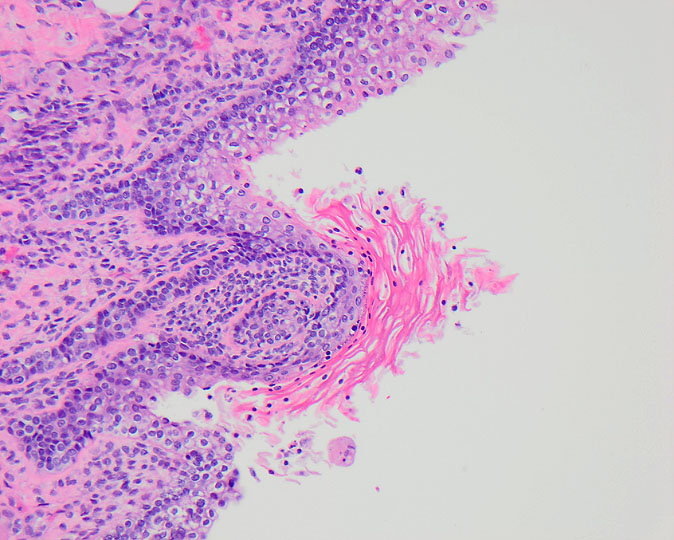
Q2. What is the vascular alteration characteristic of this disease process?
Invasive fibrous thyroiditis (IgG4-related thyroiditis; Riedel thyroiditis)
Invasive fibrous thyroiditis is a rare form of chronic thyroiditis on the spectrum of IgG4-related diseases, characterized by extensive fibrosis and increased IgG4-expressing plasma cells. The cause is unknown. Any number of organ systems may be involved by this process, most notably the pancreas. When the thyroid gland is affected, extensive replacement of the glandular tissue by fibrosis is seen histologically. Up to one third of patients with invasive fibrous thyroiditis will experience IgG4-related disease in another organ.
The condition is seen more often in women, usually in the 5th decade. There is an association with cigarette-smoking. Patients usually present with a very firm goiter, often with compressive symptoms. Extensive fibrosis may damage the recurrent laryngeal nerve, causing vocal cord paralysis and hoarseness. The sympathetic trunk may also be affected, resulting in Horner syndrome. Occlusion of blood vessels and destruction of parathyroid glands may occur. Invasive fibrous thyroiditis may mimic malignancy clinically due to infiltration of the fibrosis into the soft tissues of the neck.
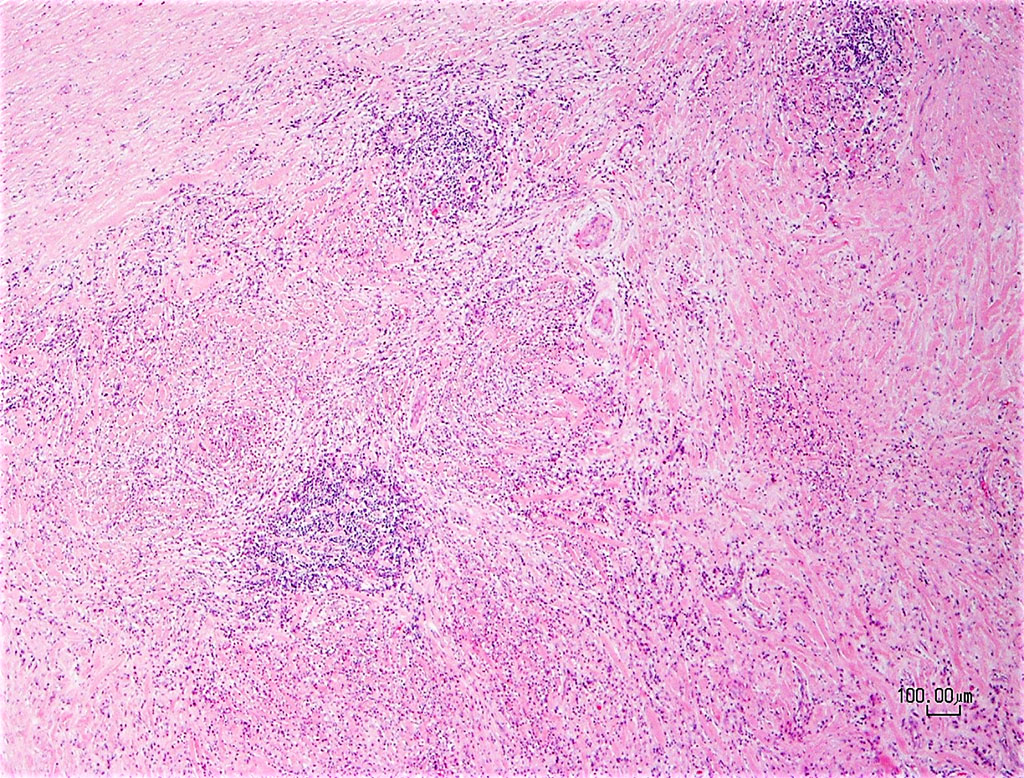
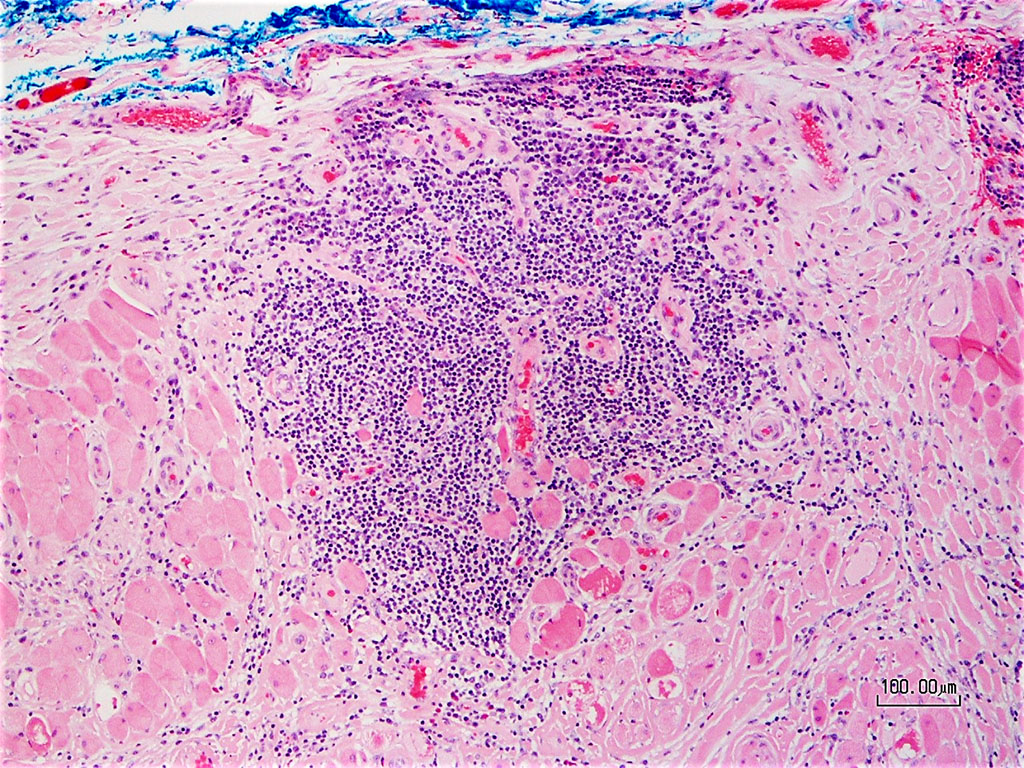
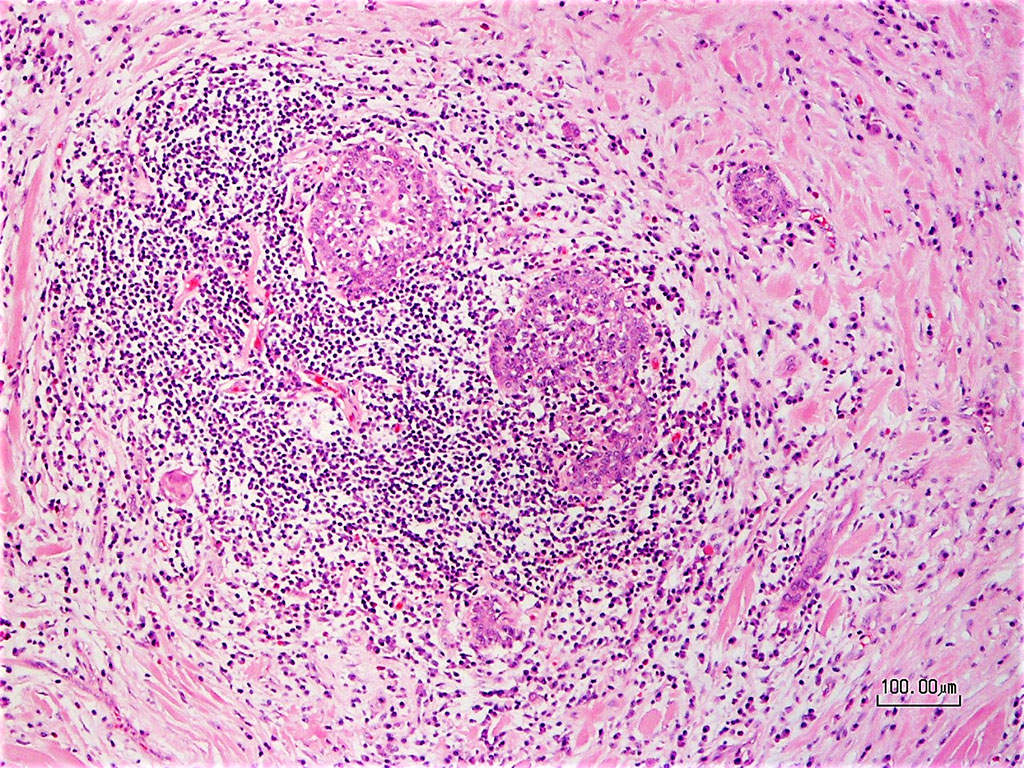
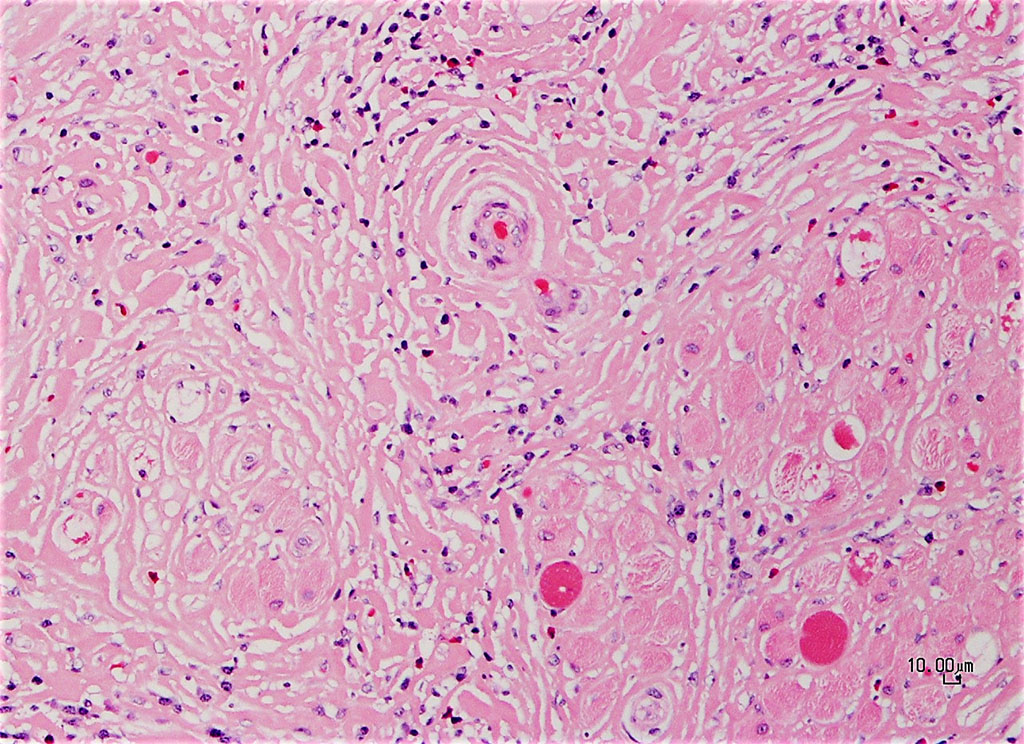
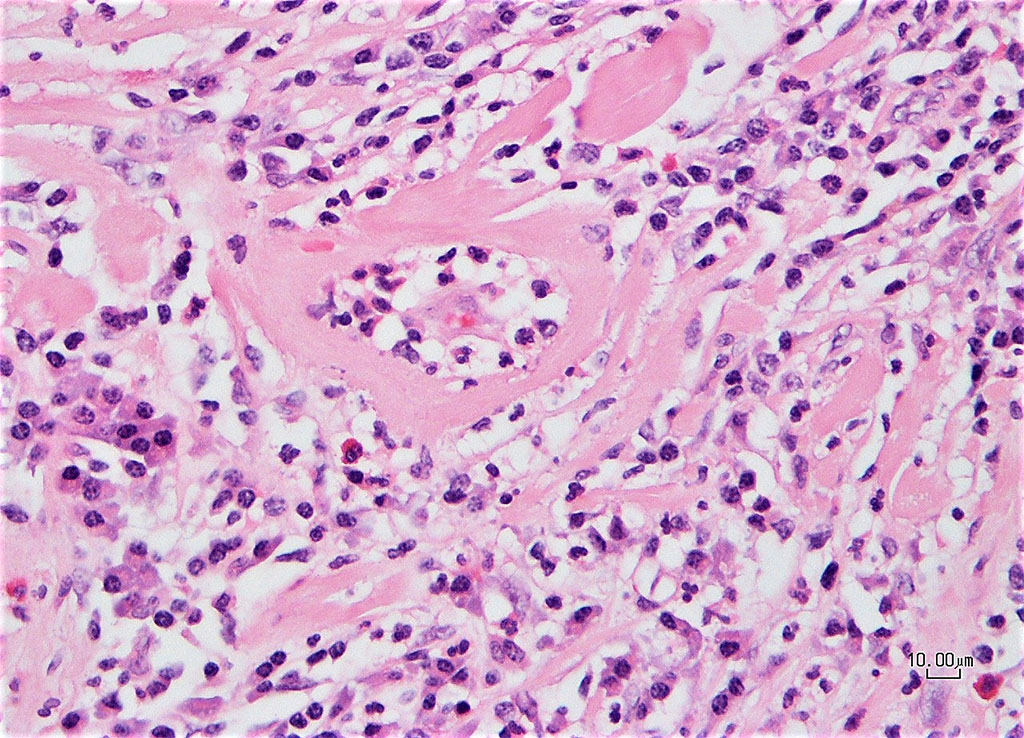
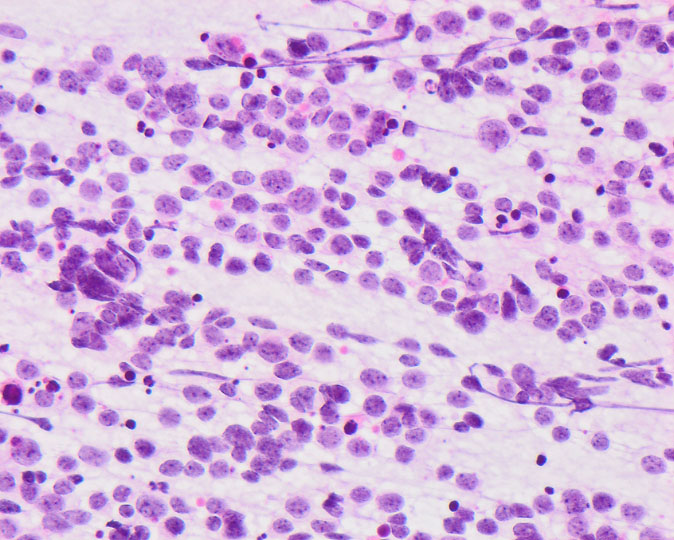
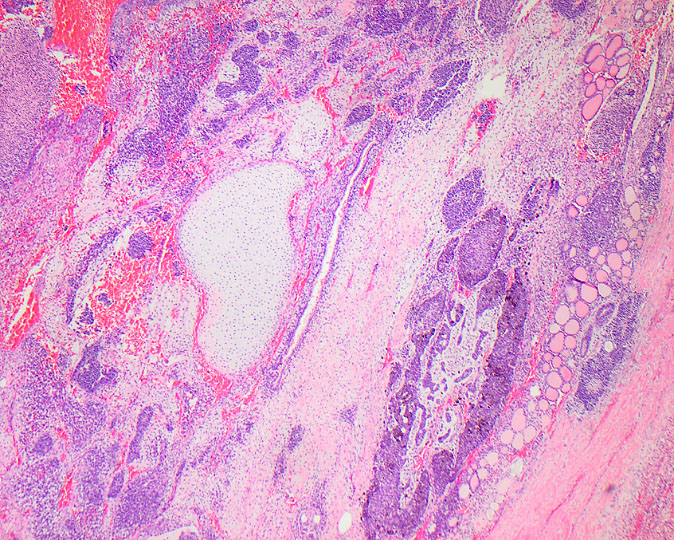
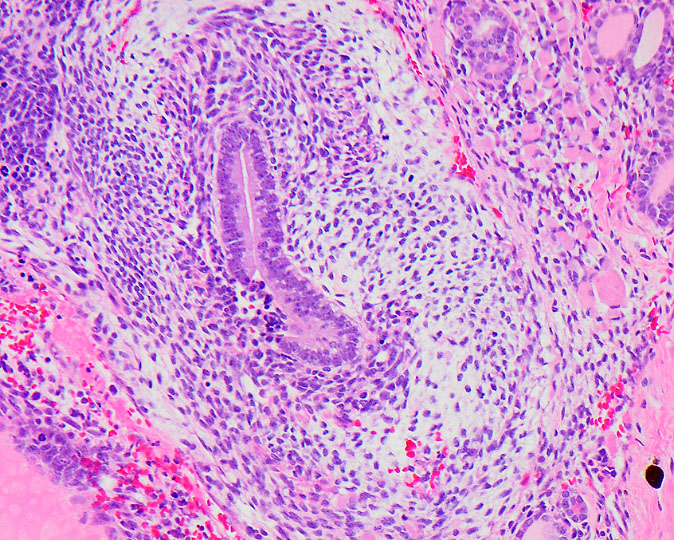
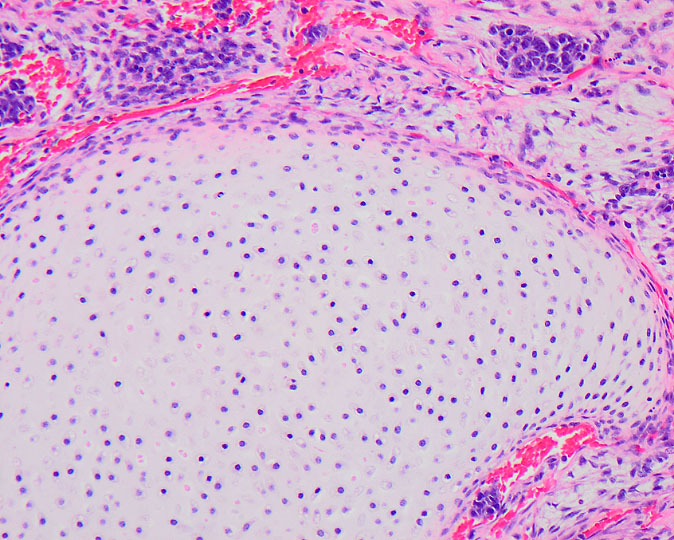
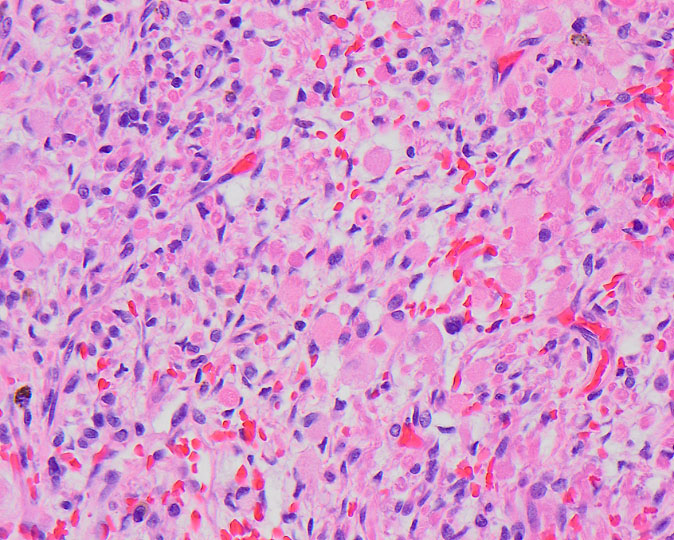
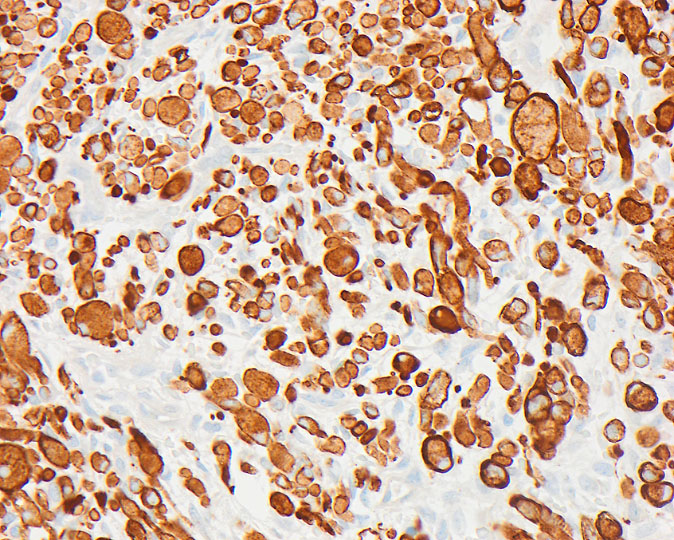
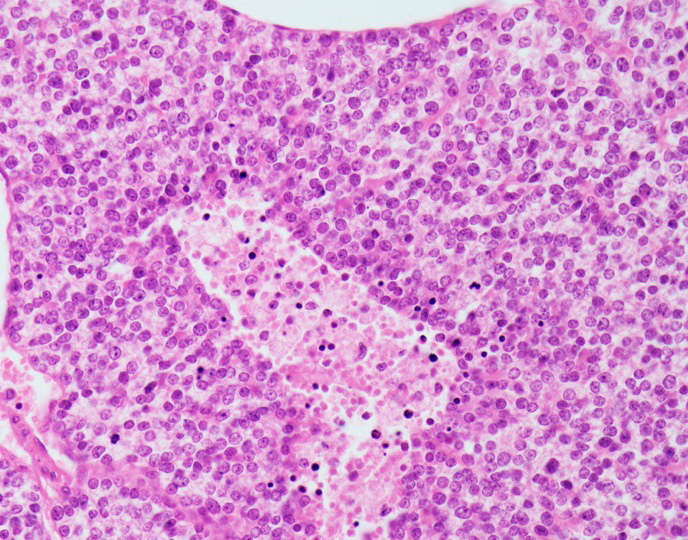
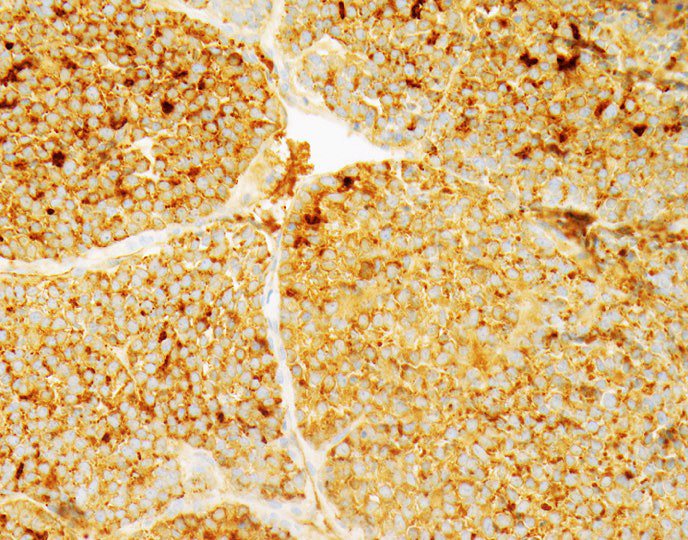
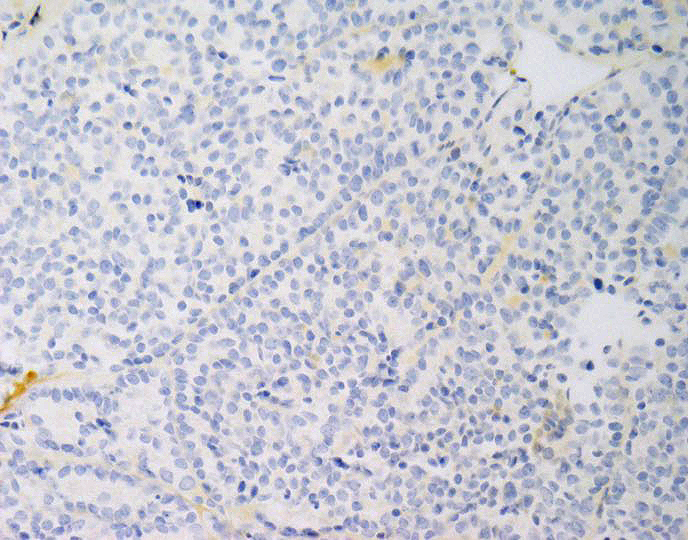
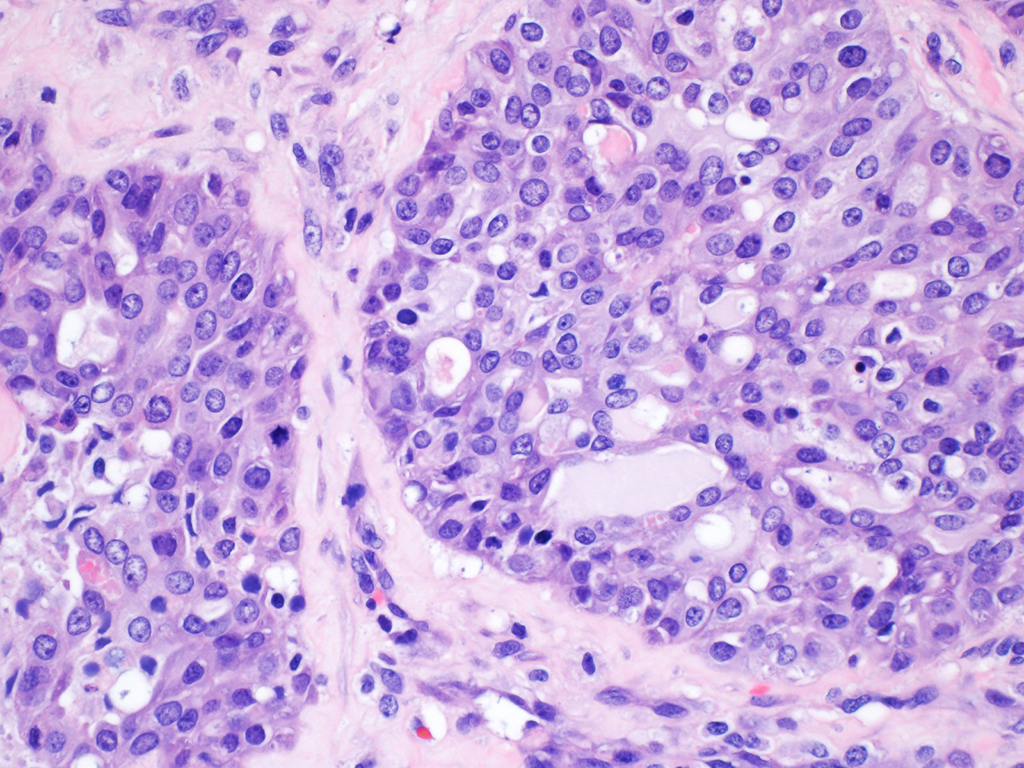
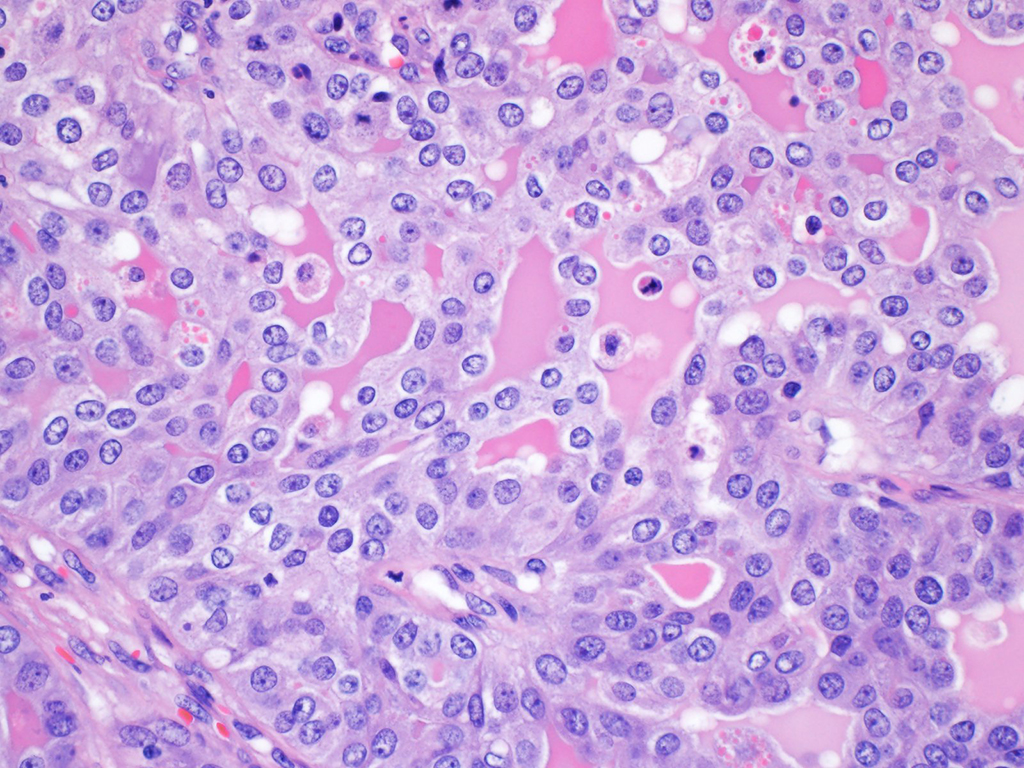
Microscopic examination reveals fibrosis overtaking the thyroid gland in broad hypocellular zones, with associated patchy chronic inflammation. Some residual atrophic thyroid follicles may remain, but extensive fibrous replacement is typical. Extension into the soft tissue and strap muscles results in fixation of the mass. Occlusive phlebitis (characteristic of IgG4-related disease), or fibrosis and inflammation of small and medium veins, is noted in most cases.
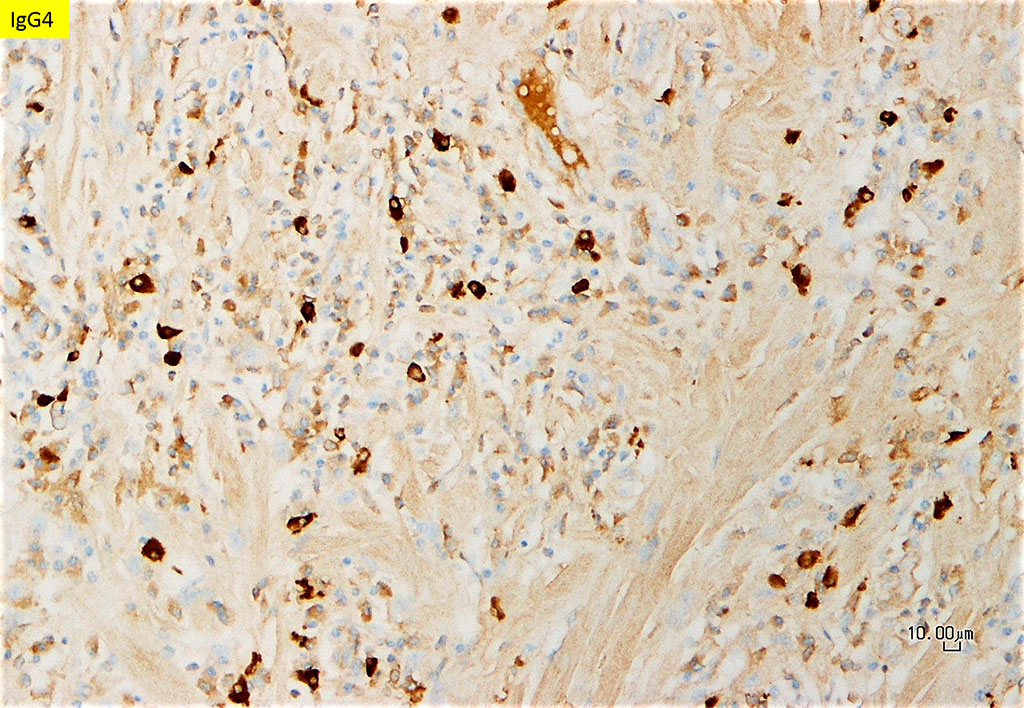
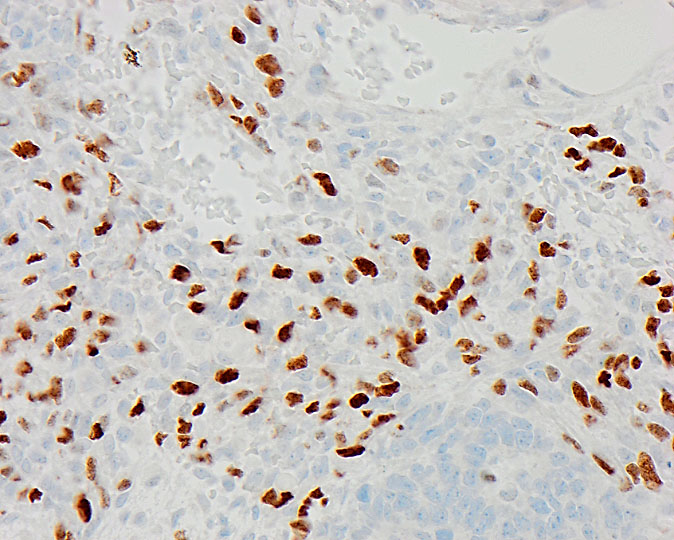
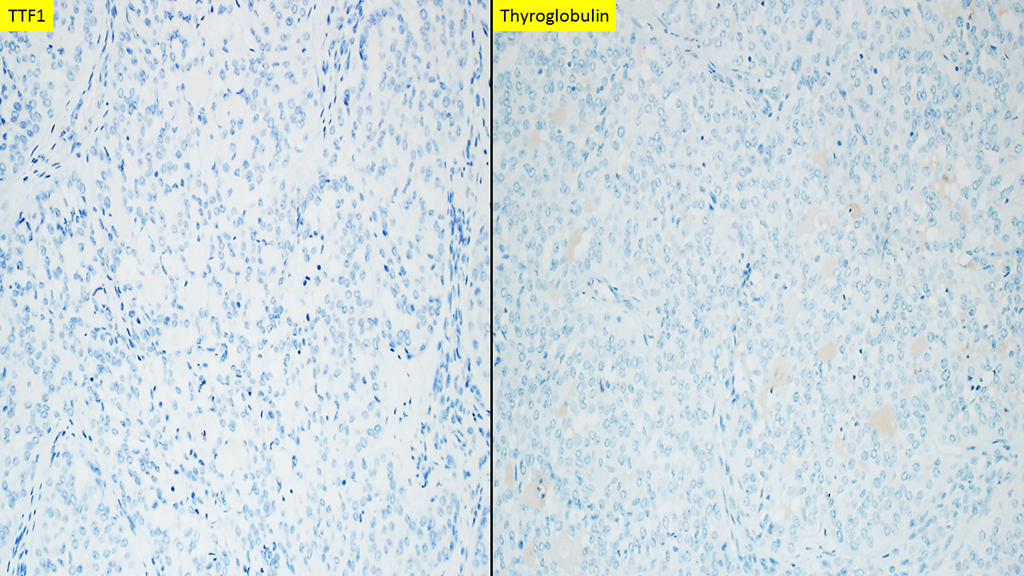
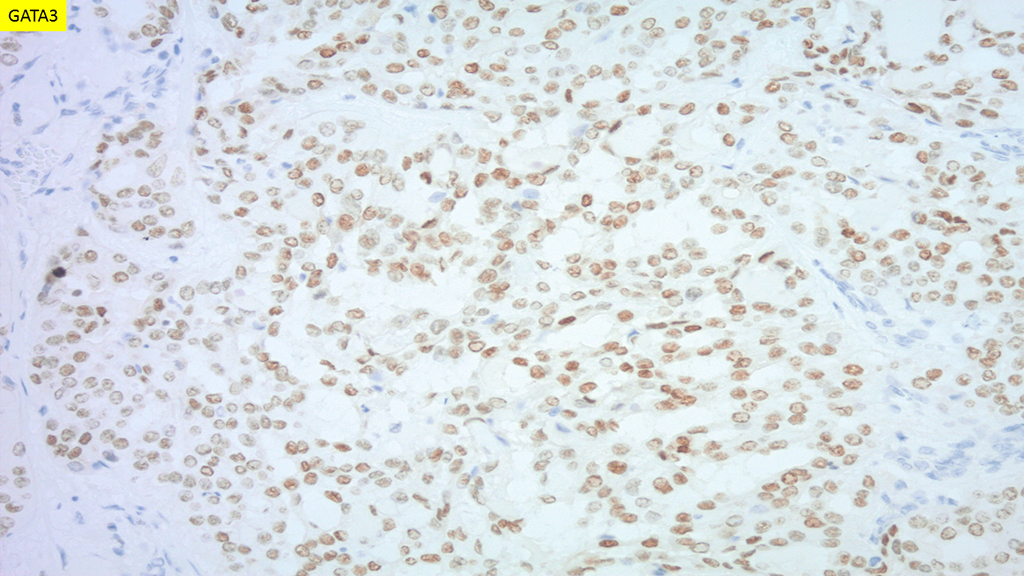
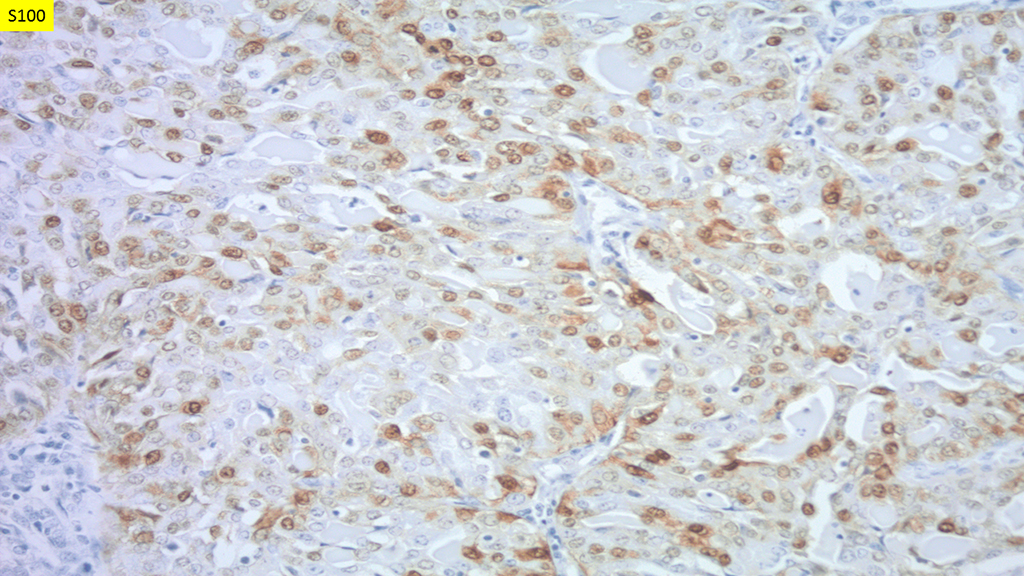
Elevated serum IgG4 levels are present only in about 50% of patients, and this finding is not specific to invasive fibrous thyroiditis, so it is of somewhat limited diagnostic value. Immunohistochemistry for IgG and IgG4 is helpful if it demonstrates an increased ratio of IgG4 to IgG-expressing plasma cells: a ratio of greater than 40% is supportive of this diagnosis. Hypothyroidism and/or hypoparathyroidism are typical sequelae of invasive fibrous thyroiditis.
While it may act aggressively, invasive fibrous thyroiditis is a benign condition and does not always require surgical treatment. Medical management of hypothyroidism and/or hypoparathyroidism is needed in affected patients. Patients should be monitored for manifestations of IgG4-related disease in other organ systems, as systemic involvement is associated with significant morbidity and mortality. Corticosteroid therapy is useful in such situations.
References
- Falhammar H, Juhlin CC, Barner C, Catrina SB, Karefylakis C, Calissendorff J. Riedel’s thyroiditis: clinical presentation, treatment and outcomes. Endocrine. 2018;60(1):185-192. doi:10.1007/s12020-018-1526-3
- Mammen SV, Gordon MB. SUCCESSFUL USE OF RITUXIMAB IN A CASE OF RIEDEL THYROIDITIS RESISTANT TO TREATMENT WITH PREDNISONE AND TAMOXIFEN. AACE Clin Case Rep. 2019;5(3):e218-e221. Published 2019 Apr 25. doi:10.4158/ACCR-2018-0352
- Darouichi M, Constanthin PE. Riedel’s thyroiditis. Radiol Case Rep. 2016;11(3):175-177. Published 2016 Jun 17. doi:10.1016/j.radcr.2016.05.017
- Thompson LDR, Bishop JA. (2019). Head and Neck Pathology, 3rd edition, pp 557-561. Philadelphia, PA: Elsevier.
Quiz Answers
Q1 = C. Serum IgG4
Q2 = D. Occlusive phlebitis
Anne C. McLean-Holden, DMD, MS: Emory University Hospital, Atlanta, GA
Justin A. Bishop, MD: University of Texas Southwestern Medical Center, Dallas, TX