A middle-aged man presented with a palpable neck mass and was found to have a complex 8.5 cm mass arising from the left thyroid lobe. He had no notable past medical history and no history of radiation exposure. The patient underwent hemithyroidectomy, with negative margins. Following resection, staging PET/CT/ultrasound did not demonstrate any other lesions.
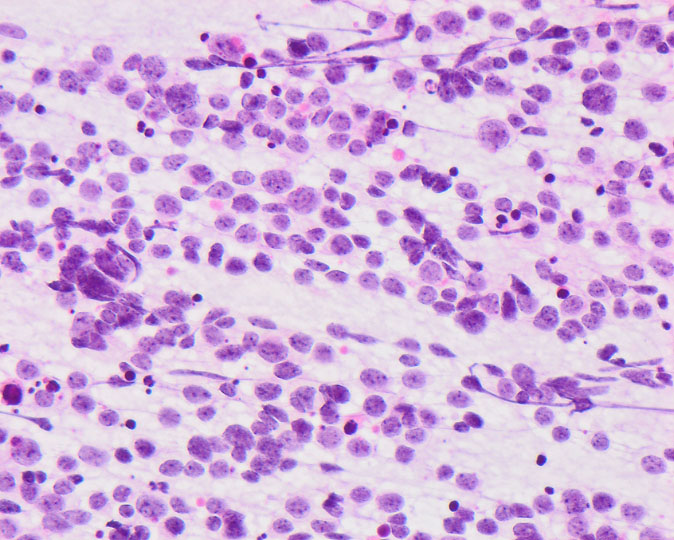
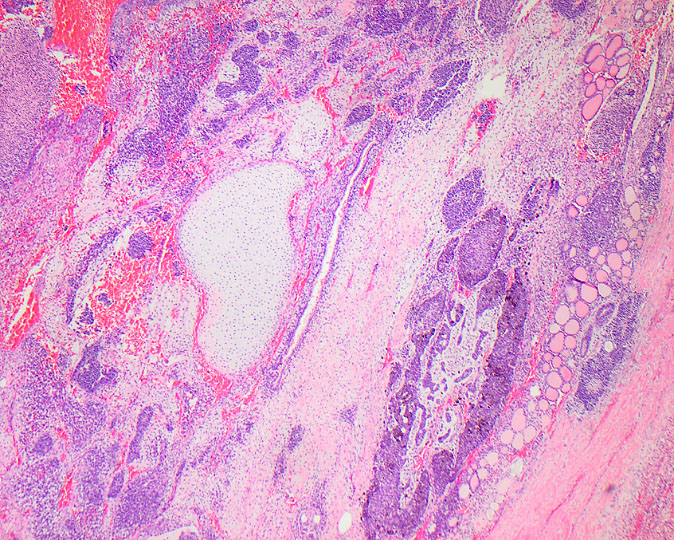
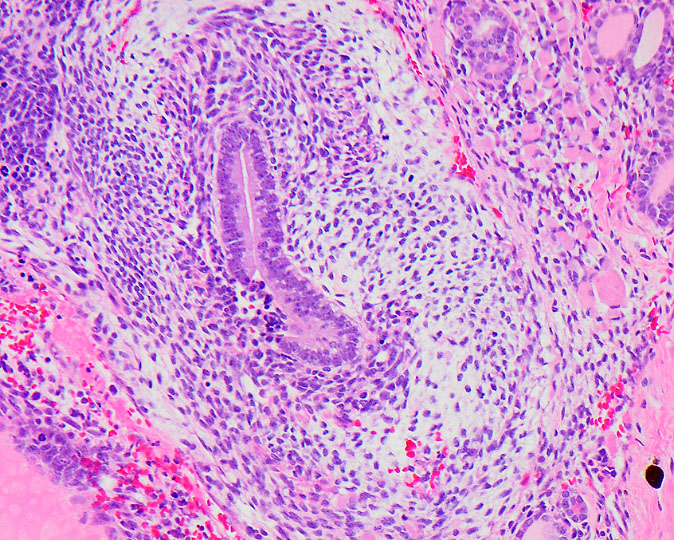
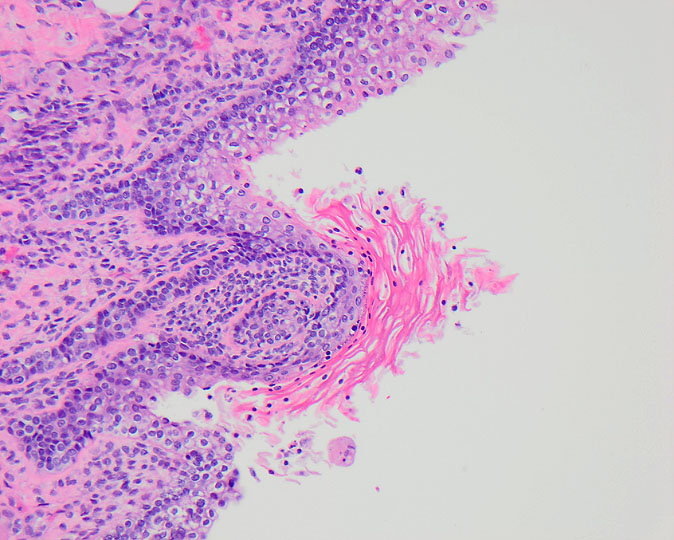
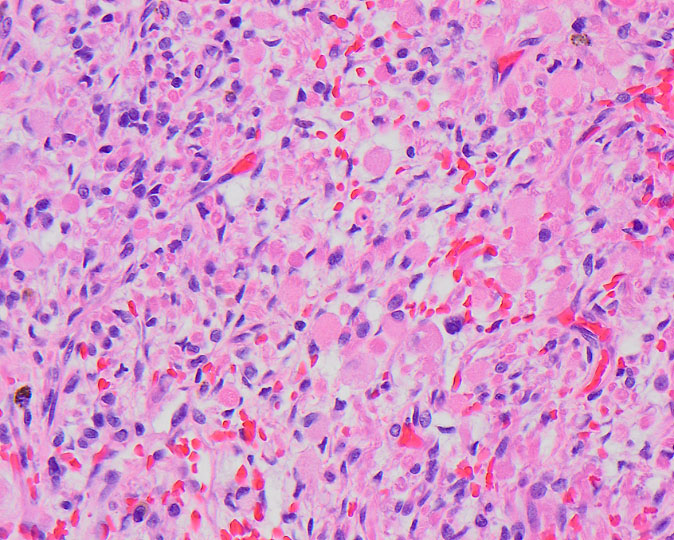
Two months after hemithyroidectomy, the patient developed neck and supraclavicular swelling. PET/CT demonstrated a mass in the surgical bed extending into the mediastinum, as well as nodules in the contralateral platysma, sternocleidomastoid muscle, and supraclavicular region. A fine needle aspiration was performed of a palpable supraclavicular nodule. Images from the supraclavicular fine needle aspiration and thyroid resection are shown.
Q1. Which genetic alteration has been associated with this tumor?
Q2. Tumors occurring in infants and children generally have a favorable prognosis.
Malignant Thyroid Teratoma.
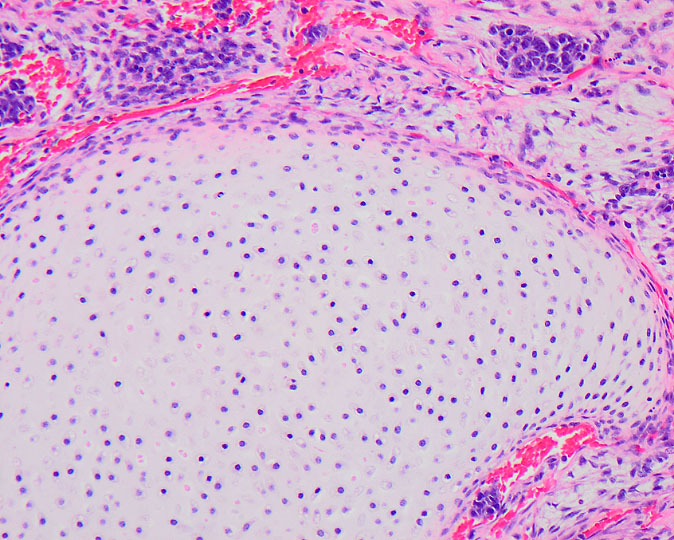
Primary thyroid teratomas are rare neoplasms that, like gonadal teratomas, are defined by the presence of tissues derived from the 3 embryonic germ layers (ectoderm, mesoderm, and endoderm). However, in contrast to gonadal teratomas which may occur as a component in a mixed germ cell tumor, there have not been any reported cases of thyroid teratoma co-occurring with other subtypes of germ cell tumor. Furthermore, primary thyroid teratomas lack isochromosome 12p, so appear to be genetically distinct from teratomas of other sites.
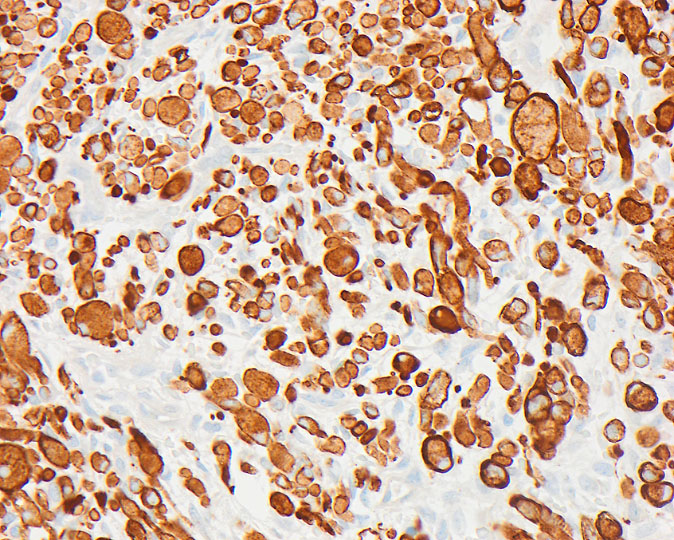
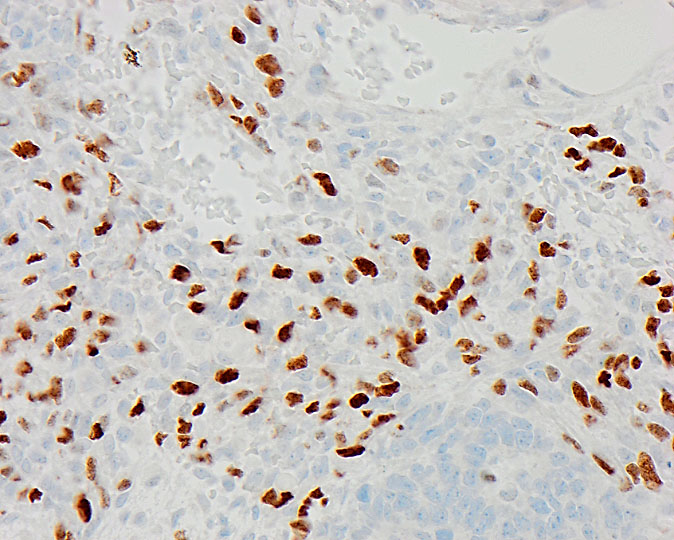
A grading scheme proposed by Thompson et al. divides thyroid teratomas into three categories: benign, immature, and malignant. Benign teratomas contain exclusively mature elements. Immature elements are defined as tissues resembling embryonic components, most commonly immature neural elements. Immature teratomas contain immature elements occupying <4 low power fields, while malignant teratomas contain ≥4 low-power fields of immature tissues. Rooper et al. noted that not all malignant teratomas contained immature neural elements, but instead may show a predominance of primitive epithelial and/or spindled elements. The immature spindled areas often may have rhabdomyosarcomatous differentiation which express desmin and myogenin, a feature that is seen in the current case. Immunohistochemistry is often not required for diagnosis given the characteristic histologic features but may be useful in small biopsies or fine needle aspiration specimens. The tumors generally have TTF-1 and PAX-8 expression, with pancytokeratin positivity in the epithelial components and synaptophysin positivity in the immature neural elements.
Thyroid teratomas affect a wide age range and have a variable clinical course depending on histologic grade. Benign and immature teratomas of the thyroid are found in infants and young children and may occur congenitally. If surgical excision is possible, benign and immature teratomas generally have an excellent prognosis, with no reported cases of local recurrence or metastatic disease after complete excision. Despite favorable histology, congenital teratomas have been documented to be fatal due to tracheal compression and/or lack of normal neck development. Malignant teratomas are more common in adults and often behave aggressively, with a potential for local recurrence and distant metastases. Malignant teratomas have been shown to have recurrent DICER1 mutations, while these mutations were absent in tumors with benign/immature histology. The dissimilar molecular profile, along with the differences in clinical outcome and age at presentation, suggests that malignant teratoma may represent a distinct pathologic entity, as opposed to existing on a spectrum with benign/immature teratoma.
References
- Rooper LM, Bynum JP, Miller KP, et al. Recurrent DICER1 Hotspot Mutations in Malignant Thyroid Gland Teratomas: Molecular Characterization and Proposal for a Separate Classification. Am J Surg Pathol. 2020;44(6):826‐833. doi:10.1097/PAS.0000000000001430
- Agaimy A, Witkowski L, Stoehr R, et al. Malignant teratoid tumor of the thyroid gland: an aggressive primitive multiphenotypic malignancy showing organotypical elements and frequent DICER1 alterations-is the term “thyroblastoma” more appropriate? [published online ahead of print, 2020 Jun 7]. Virchows Arch. 2020;10.1007/s00428-020-02853-1. doi:10.1007/s00428-020-02853-1
- Thompson LD, Rosai J, Heffess CS. Primary thyroid teratomas: a clinicopathologic study of 30 cases. Cancer. 2000;88(5):1149‐1158.
- Miller DL, Thompson LDR, Bishop JA, Rooper LM, Ali SZ. Malignant teratomas of the thyroid gland: clinico-radiologic and cytomorphologic features of a rare entity [published online ahead of print, 2020 Apr 28]. J Am Soc Cytopathol. 2020;S2213-2945(20)30070-3. doi:10.1016/j.jasc.2020.04.008
Quiz Answers
Q1 = A. DICER1
Q2 = A. True. Teratomas in infants and young children generally have a very favorable prognosis. Complete surgical excision is typically curative.