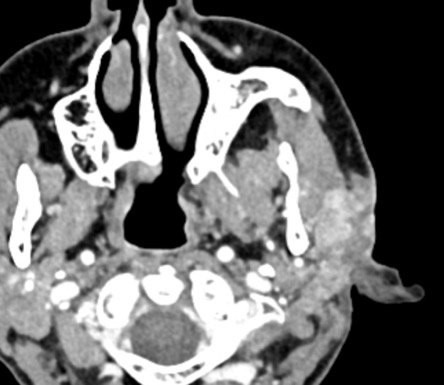
A 61-year-old female presents with an enlarging mass along the left angle of the mandible and pre-auricular area. A contrast-enhanced CT scan of the neck shows a heterogeneous, irregular left preauricular mass involving the parotid gland and invading into facial skin.
1. Which of the following immunohistochemical stains is MOST likely to be positive in this carcinoma?
2. Which of the following is TRUE?
Salivary duct carcinoma with squamous cell and sarcomatoid components
Salivary duct carcinoma is an epithelial malignancy that can occur de novo or as the malignant component in a carcinoma ex pleomorphic adenoma. This type of neoplasm accounts for approximately 10% of salivary gland neoplasms and most commonly arises in the parotid gland. Salivary duct carcinoma classically presents in elderly males in the sixth and seventh decades as a rapidly growing tumor usually with associated facial nerve paralysis. Several histological subtypes have been described including: micropapillary, sarcomatoid, mucinous, basal-like, and oncocytic. However, mixed cell types are very rare. The most frequent genetic alterations include mutations in TP53 (55%), HRAS (23%), PIK3CA (23%), amplification of ERBB2 (35%), PTEN deletion, and BRAF mutations.
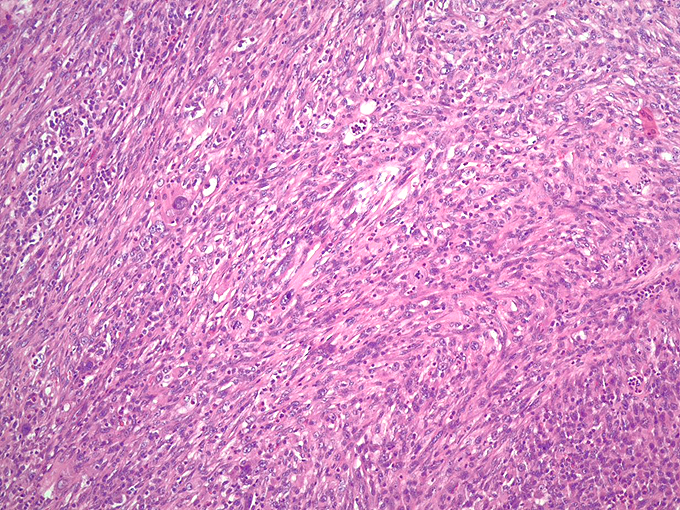
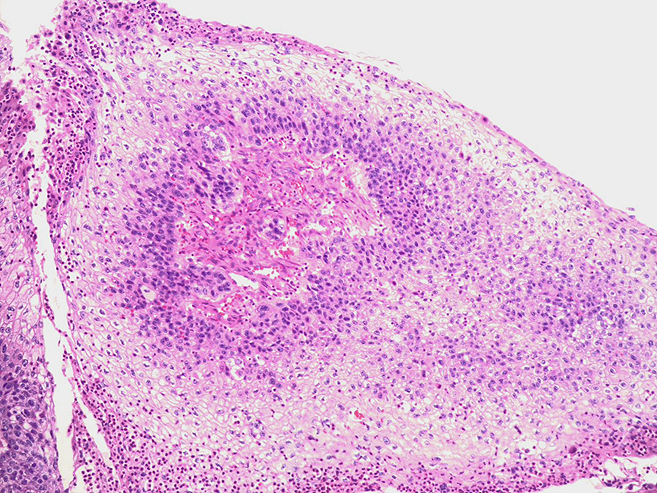
Histologically, salivary duct carcinoma resembles high-grade ductal carcinoma of the breast. Architecturally, the tumor cells in salivary duct carcinoma form large ducts with comedonecrosis, cribriforming, and Roman-bridge-like features (Figures 2 and 3). Cytologically, tumor cells have apocrine and oncocytic features with abundant, eosinophilic cytoplasm and round nuclei with vesicular chromatin and prominent nucleoli. Nuclear pleomorphism and mitotic figures are common. When salivary duct carcinoma has a mixed cell type such as sarcomatoid (Figure 4), the components are usually distinct, but a transition zone may be present. Squamous cell carcinoma mixed with salivary duct carcinoma has been very rarely described (Figures 2 and 5).
Classically, the majority of salivary duct carcinomas stain positive for androgen receptor. As seen in our case of a mixed cell type carcinoma, immunohistochemistry shows distinct staining in the salivary duct carcinoma and squamous cell components (Figures 6 and 7). The salivary duct carcinoma component is strongly and diffusely positive for androgen receptor and almost totally negative for p40, while the squamous cell carcinoma component is strongly and diffusely positive for p40 and negative for androgen receptor. Salivary duct carcinoma is one of the most aggressive types of salivary gland carcinoma with a median overall survival of 69 months and a disease specific survival of 64% from a large SEER analysis. Subtypes, including the sarcomatoid subtype, aren’t clearly associated with worse outcomes, but the clinical significance of this extremely rare mixed squamous cell carcinoma component is unknown.
References
- WHO Classification of Tumours Editorial Board. Head and neck tumours. Lyon (France): International Agency for Research on Cancer; forthcoming. (WHO classification of tumours series, 5th ed.; vol. 9). https://publications.iarc.fr.
- Hardy N, Thompson J, Mehra R, Drachenberg CB, Hatten K, Papadimitriou JC. Parotid Salivary Duct Carcinoma With a Prominent Squamous Component: Immunohistochemical Profile, Diagnostic Pitfalls, and Therapeutic Implications. Int J Surg Pathol. 2021;29(7):726-730.
- Kusafuka K, Kawasaki T, Onitsuka T, Hamaguchi N, Morita K, Mukaigawa T, Nishiya Y, Kamijo T, Iida Y, Nakajima T, Sugino T. Acantholytic Squamous Cell Carcinoma and Salivary Duct Carcinoma Ex-pleomorphic Adenoma of the Submandibular Gland: A Report of Two Extremely Rare Cases with an Immunohistochemical Analysis. Head Neck Pathol. 2020;14(1):230-238.
- Nagao T, Gaffey TA, Serizawa H, Iwaya K, Watanabe A, Yoshida T, Yamazaki K, Sageshima M, Lewis JE. Sarcomatoid variant of salivary duct carcinoma: clinicopathologic and immunohistochemical study of eight cases with review of the literature. Am J Clin Pathol. 2004;122(2):222-31.
- Williams L, Thompson LD, Seethala RR, Weinreb I, Assaad AM, Tuluc M, Ud Din N, Purgina B, Lai C, Griffith CC, Chiosea SI. Salivary duct carcinoma: the predominance of apocrine morphology, prevalence of histologic variants, and androgen receptor expression. Am J Surg Pathol. 2015; 39(5):705-13.
- Jayaprakash V, Merzianu M, Warren GW, Arshad H, Hicks WL Jr, Rigual NR, Sullivan MA, Seshadri M, Marshall JR, Cohan DM, Zhao Y, Singh AK. Survival rates and prognostic factors for infiltrating salivary duct carcinoma: Analysis of 228 cases from the Surveillance, Epidemiology, and End Results database. Head Neck. 2014;36(5):694-701
Quiz Answers
Q1 = B. Androgen receptor
Q2 = D. This carcinoma can show ERBB2 gene amplification
James S. Lewis Jr. MD
Professor
Associate Director of Surgical Pathology
President, North American Society of Head and Neck Pathology
Vanderbilt University Medical Center