A 74-year-old woman presented with respiratory failure. The patient had a 3-month history of cough and progressive dyspnea with rapidly increasing neck swelling. CT Imaging revealed massive thyromegaly and lymphadenopathy with metastases to the lung, liver, kidney, and iliac bone. Patient underwent thyroid surgical resection to relieve the airway compression. Gross examination of the thyroid showed diffuse replacement by multiple masses, the largest measuring 7.6 × 5.3 × 2.7 cm, with infiltrative borders and extension into surrounding adipose tissue. H&E slides and immunostains are shown.
Q1. What is the characteristic genetic alteration in this tumor?
Q2. Adjuvant therapy with radioactive iodine would be effective.
Secretory Carcinoma of the Thyroid.
Salivary gland secretory carcinoma (SC), previously known as mammary analog secretory carcinoma, is a relatively rare neoplasm and is defined by the presence of a recurrent balanced translocation t(12:15) resulting in fusion of the ETV6 gene. These tumors were named as such due to their histologic resemblance to SC of the breast.
SC has been reported in multiple extra-salivary locations including thyroid gland and skin. Less than 20 cases of SC in the thyroid have previously been reported in the literature. The average age of presentation is 59 years (range 36–74 years) and it has a strong female predominance.
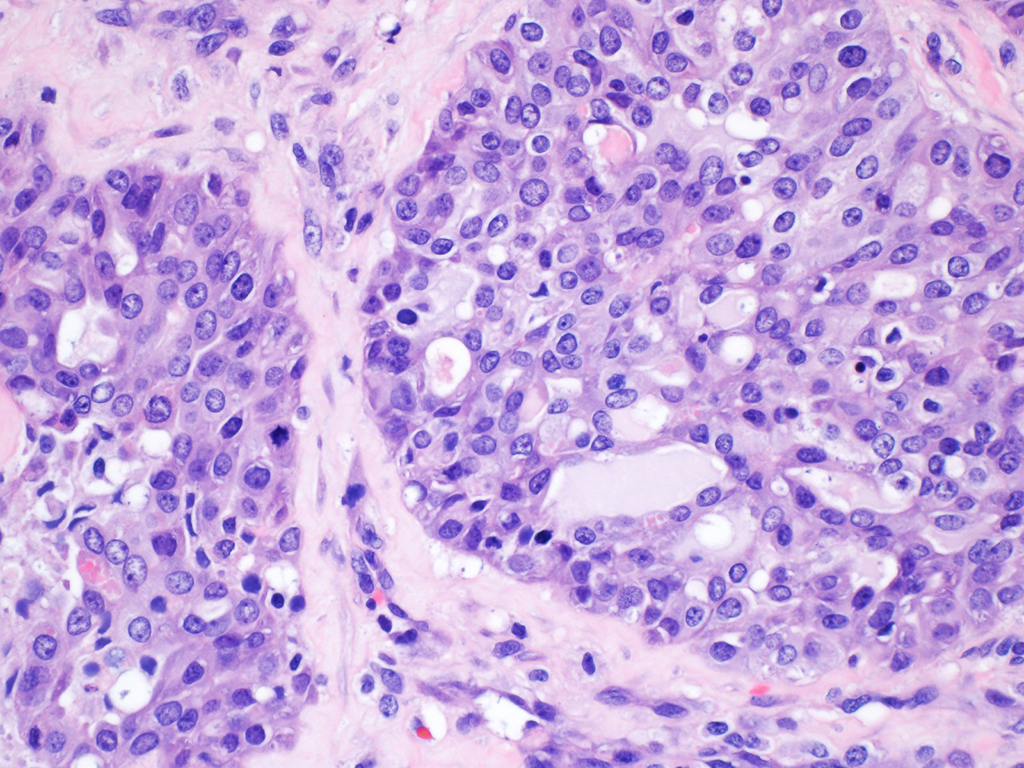
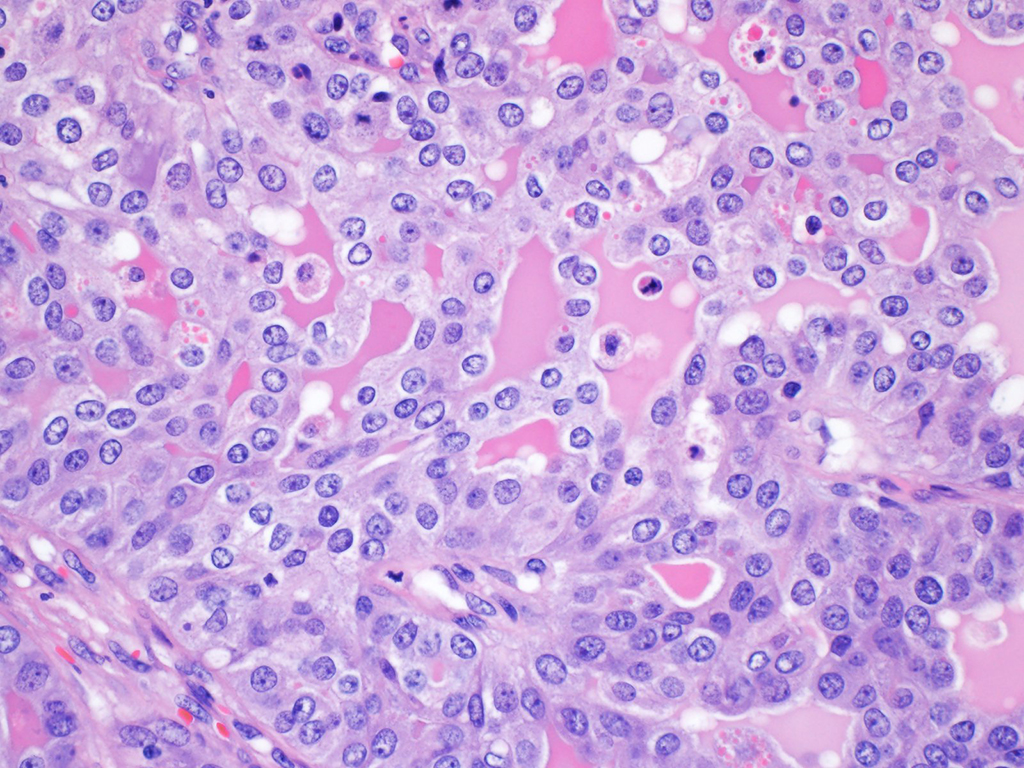
Histologically, they have a mixed microcystic, tubular, trabecular, papillary/pseudopapillary and solid growth pattern with densely hyalinized and fibrotic stroma and eosinophilic to lightly basophilic intraluminal secretions. The tumor cells are polygonal and generally uniform with low to medium nuclear-to-cytoplasmic ratio. Cytoplasm is abundant and eosinophilic and ranges from granular to bubbly or vacuolated. Nuclei are round to ovoid with vesicular chromatin. Nuclear grooves and membrane irregularities may be prominent. Pseudoinclusions are rare, but may be seen. Nucleoli are generally single, prominent and centrally located and may be eosinophilic. Necrosis and increased mitotic activity can be seen in these tumors.
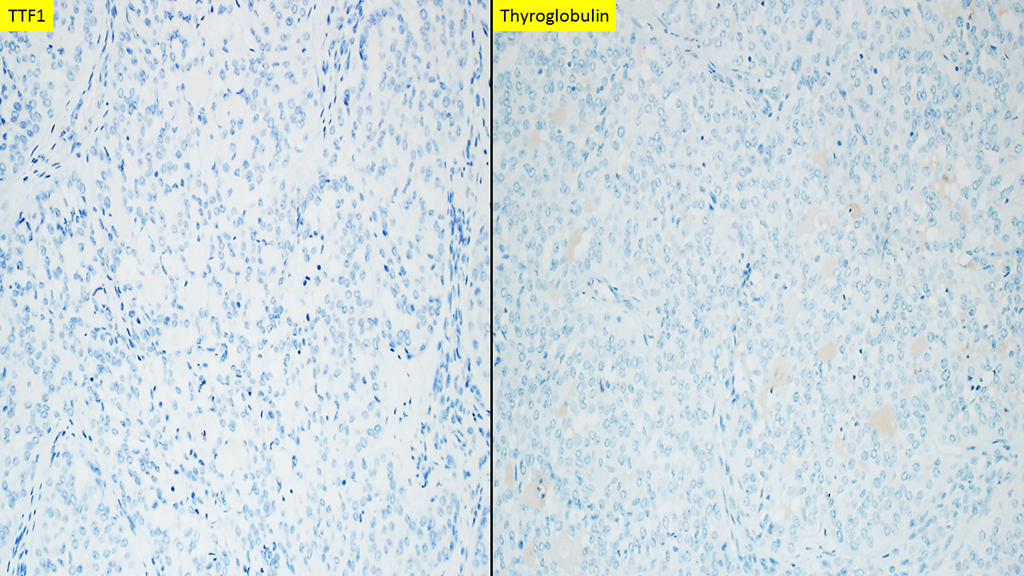
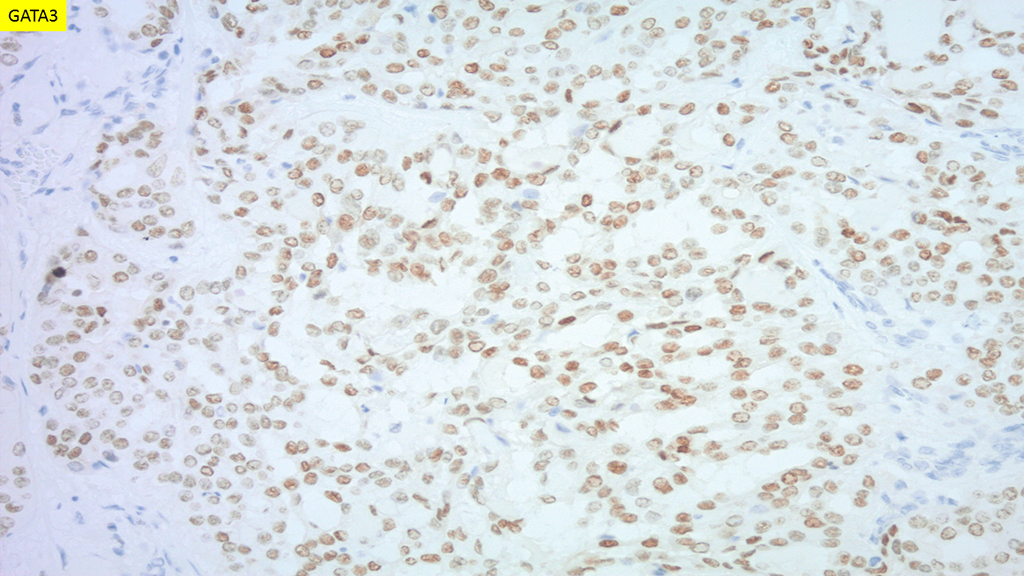
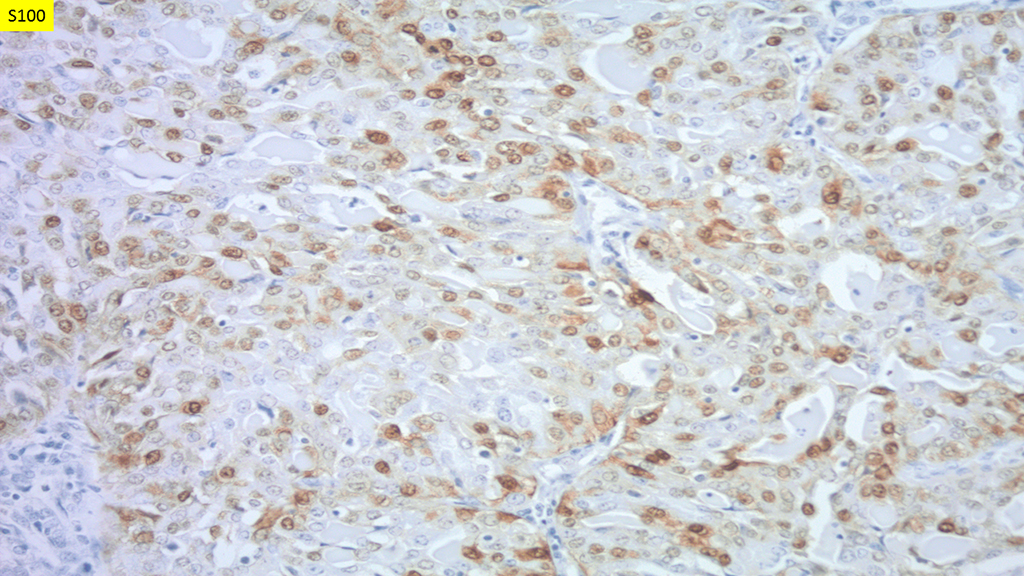
All cases of SC of the thyroid are negative for TTF-1 and Thyroglobulin while positive for mammaglobin. The majority are S100 and GATA3 positive though staining may be patchy and of variable intensity. PAX8 immunoreactivity has been reported in 90% of cases and is frequently focal and weak (Figure 6). Intraluminal secretions are positive for periodic-acid Schiff (with and without diastase) and for mucicarmine. FISH using break-apart probe for ETV6 or PCR with ETV6 and NTRK3 can be used to confirm morphologic suspicion.
Adjuvant therapy with radioactive iodine would not be effective since the tumors do not have follicular differentiation.
References
- Dettloff J, Seethala RR, Stevens TM, et al. Mammary Analog Secretory Carcinoma (MASC) Involving the Thyroid Gland: A Report of the First 3 Cases. Head Neck Pathol. 2017;11(2):124–130. doi:10.1007/s12105-016-0741-6
- Dogan S, Wang L, Ptashkin RN, et al. Mammary analog secretory carcinoma of the thyroid gland: A primary thyroid adenocarcinoma harboring ETV6-NTRK3 fusion. Mod Pathol. 2016;29(9):985–995. doi:10.1038/modpathol.2016.115
- Reynolds S, Shaheen M, Olson G, Barry M, Wu J, Bocklage T. A Case of Primary Mammary Analog Secretory Carcinoma (MASC) of the Thyroid Masquerading as Papillary Thyroid Carcinoma: Potentially More than a One Off. Head Neck Pathol. 2016;10(3):405–413. doi:10.1007/s12105-016-0715-8
Quiz Answers
Q1 = A. t(12;15)(p13,q25) ETV6-NTRK3
Q2 = B. False
Mitra Mehrad, M.D.
Assistant Professor
Department of Pathology, Microbiology and Immunology
Vanderbilt University Medical Center, Nashville, TN