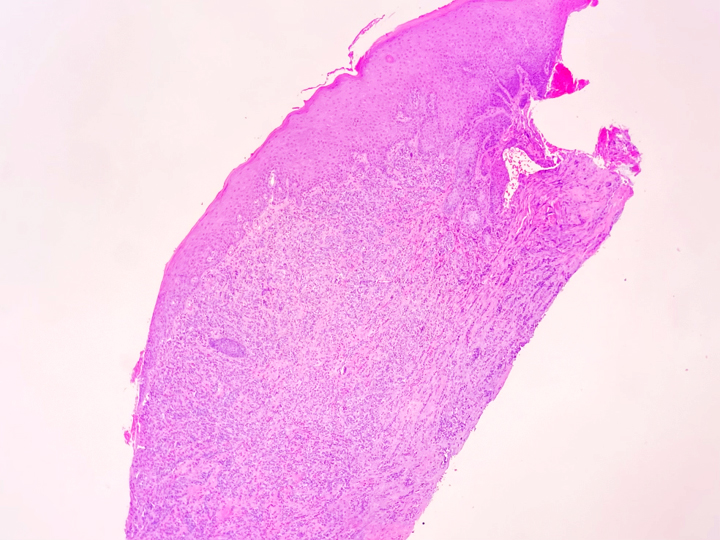
A 61-year-old female presented with a lesion on the right maxillary gingiva. Clinical examination revealed an ulcerated and endophytic lesion with associated leukoerythroplakia, involving the right maxillary gingiva and the adjacent soft tissue with noticeable bone loss. No lymphadenopathy was noted. An incisional biopsy was performed.
1. The histologic features are suggestive of:
2. True or False: The prognostic role of eosinophilic infiltration in this disease is still unknown
Squamous Cell Carcinoma
Squamous cell carcinoma (SCC) is always an important entity to consider in the differential diagnosis of any unexplained lesion in the oral cavity. SCC is the most common malignancy of the oral cavity. It typically exhibits a peak incidence in the elderly with an established relationship with tobacco and/or alcohol abuse. About 50,000 cases of oral and oropharyngeal SCC are diagnosed annually and approximately 11,000 people die of this disease each year in the US.
Oral SCC is usually slow-growing and has a varied clinical presentation, often appears as leukoplakic and/or erythroplakic lesions especially in the early course of the disease or as a fungating ulcerated mass. Greater than 50% of intraoral cancers occur on the tongue, with 2/3 of these presenting on the posterior lateral border and another 20% on the anterior lateral or ventral surfaces. The floor of the mouth is the next most common location accounting for about 1/3 of the cases. Other involved sites are soft palate, gingiva, buccal mucosa, labial mucosa, and hard palate in descending order of frequency. Therefore, SCC arising from the gingiva or alveolar ridge is a bit unusual. These SCCs occur most frequently on the attached gingiva and keratinized edentulous tissues in the posterior regions of the mandible. Most importantly gingival SCC often clinically mimics gingivitis or periodontal disease. Loosening of the involved teeth which necessitate extraction, is a frequent clinical scenario. Eventually, the socket fails to heal, and hyperplastic tissues would be noted.
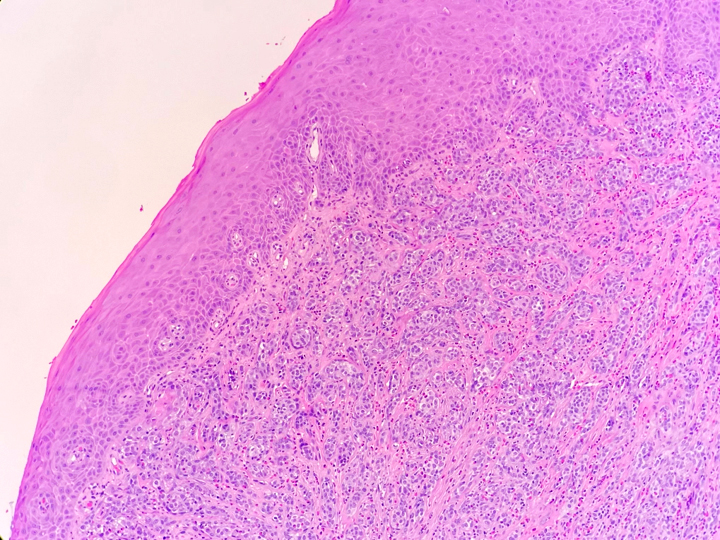
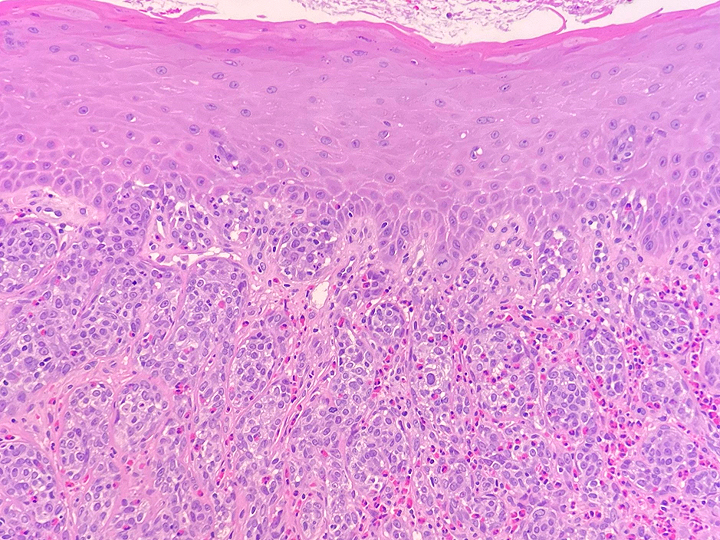
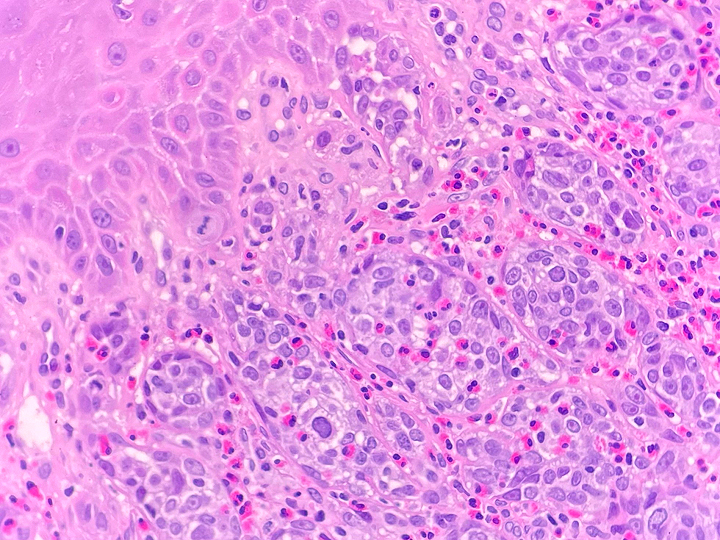
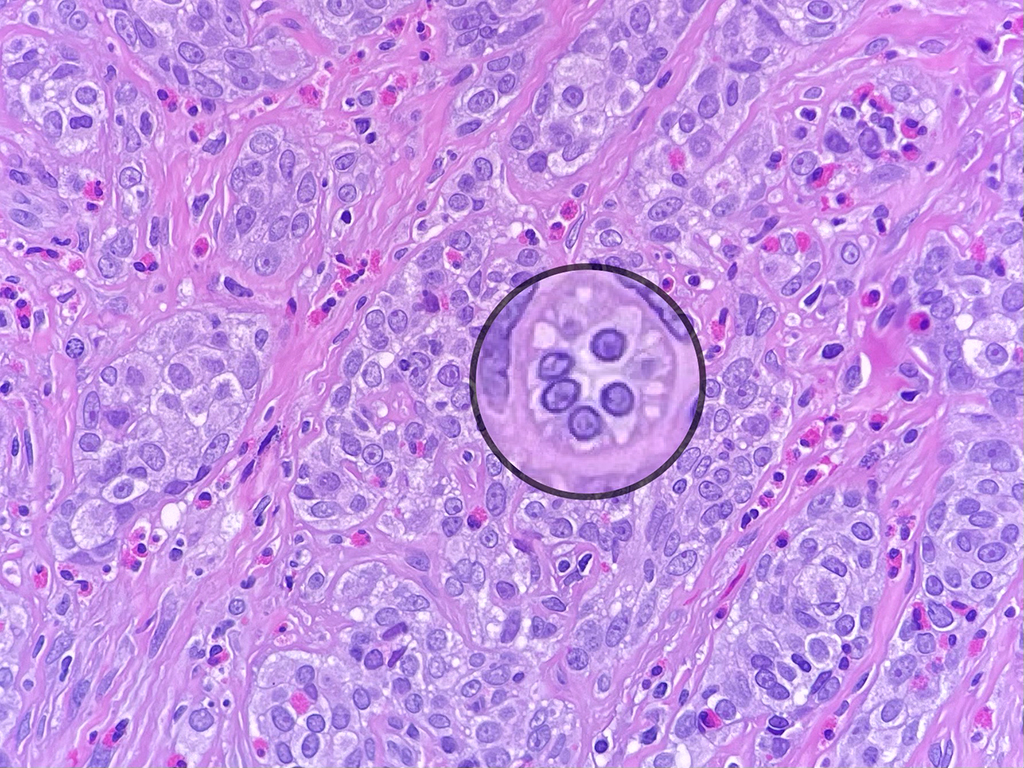
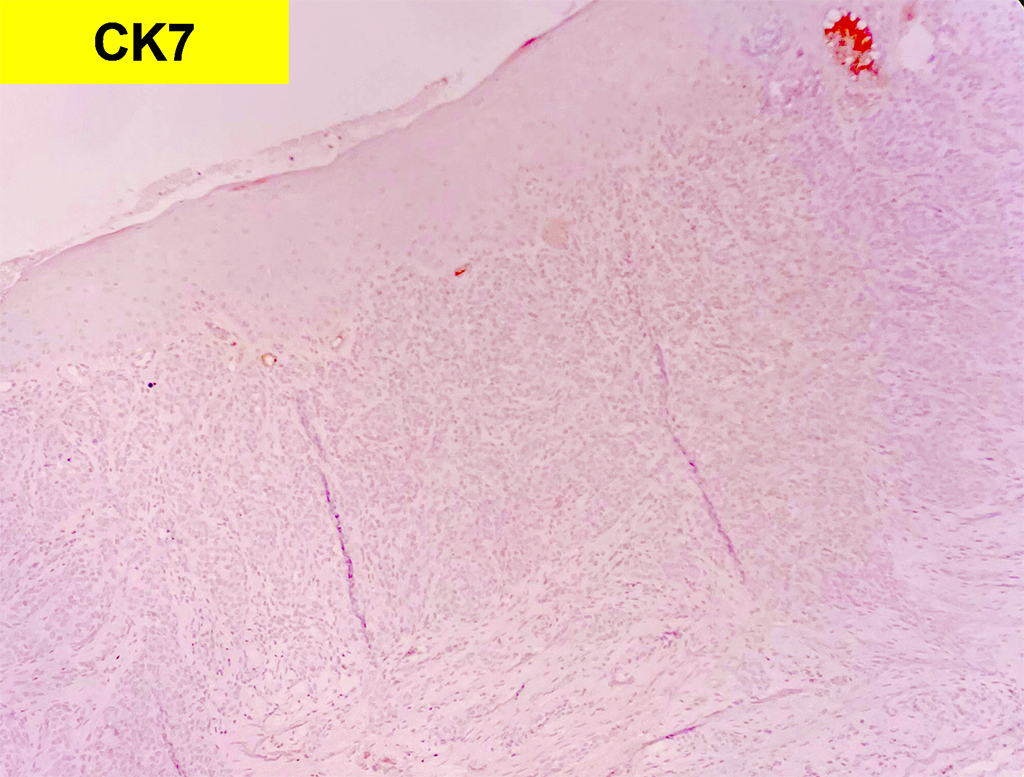
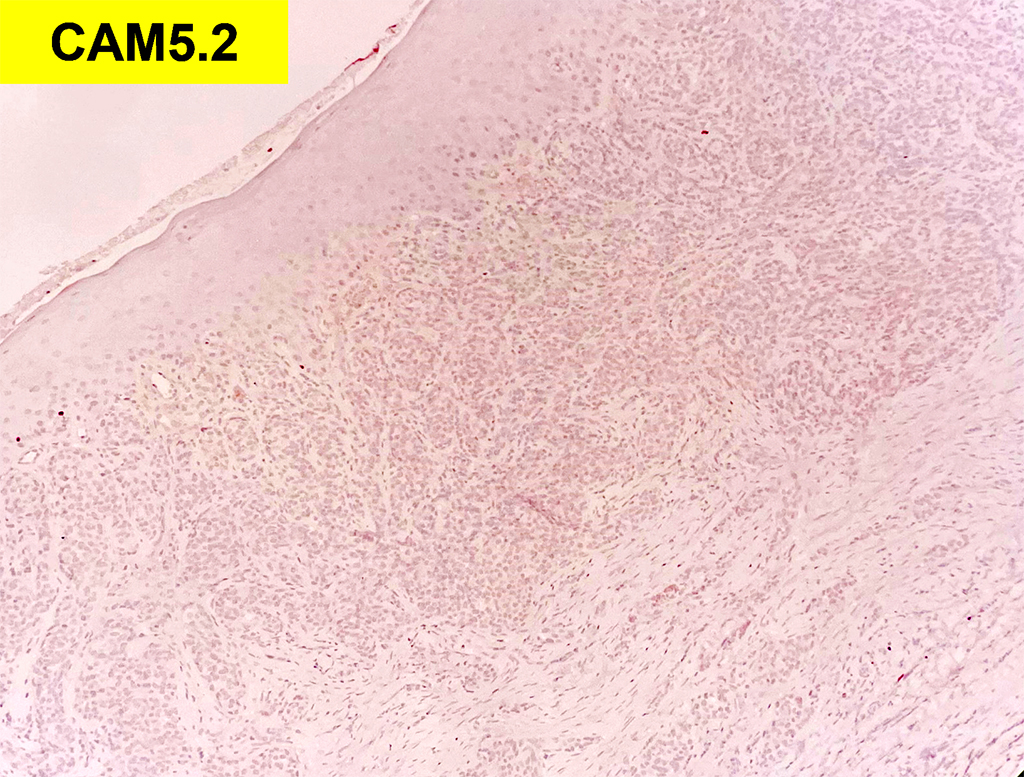
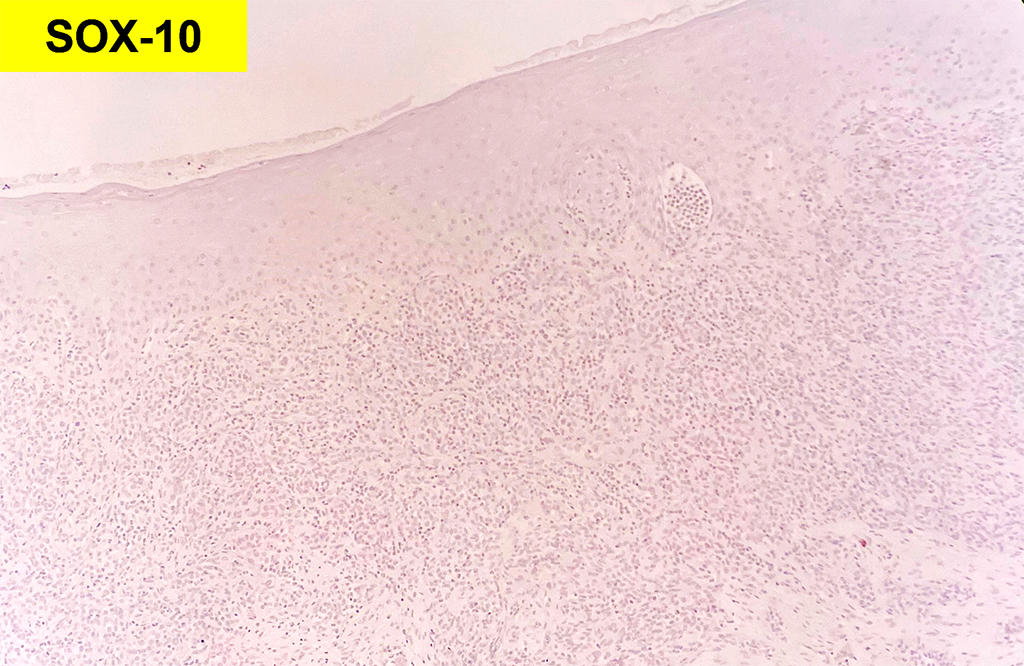
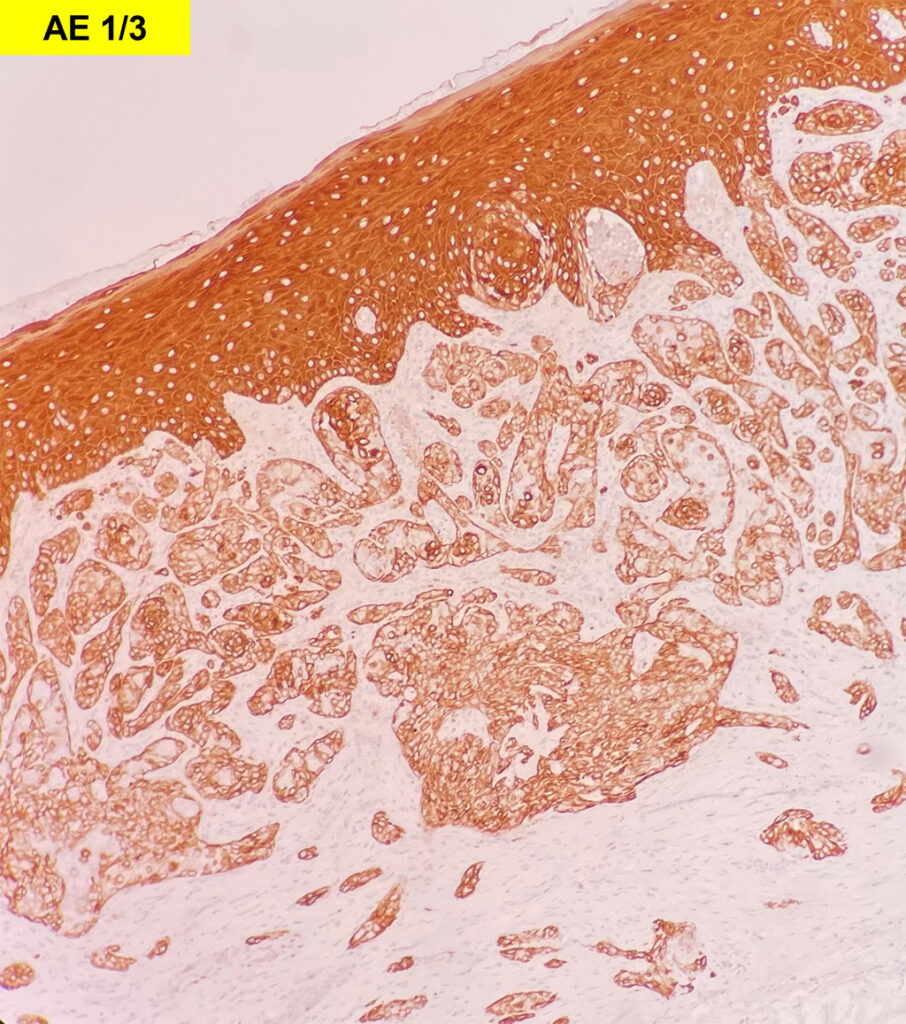
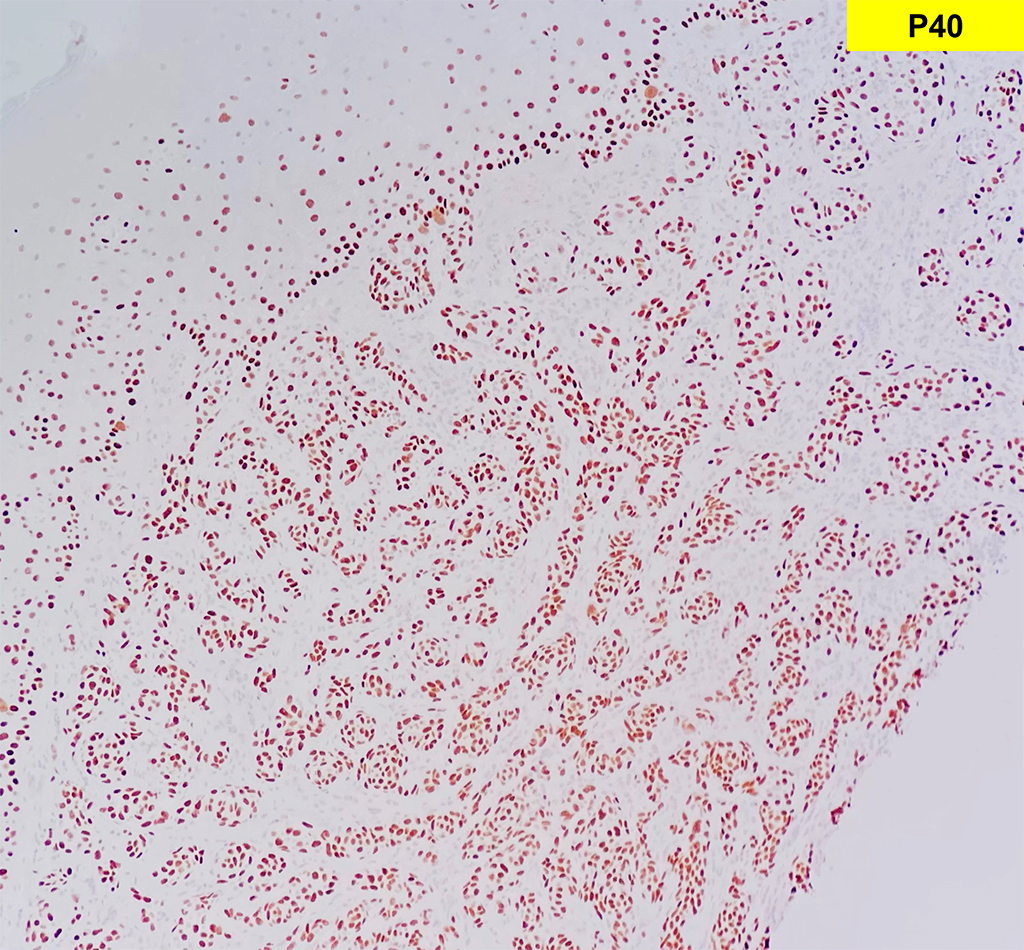
The most intriguing feature of this case is the histological findings of malignant neoplastic cells arranged in an almost theques-like pattern seen in melanoma. The neoplastic cells lack dyskeratosis. The invasive process elicits an inflammatory cell response, but marked eosinophilia is noted. Immunohistochemistry stains for melanoma were negative, however, AE1/3 and p40 were positive within lesional cells.
Lowe and Fletcher were the first to study the role of tissue eosinophilia in oral SCC in 1984. Falconieri (2008) suggested the eosinophilic-rich squamous cell carcinoma as a possible new microscopic entity of SCC. Several studies suggest an association between tissue eosinophilia and invasive SCC, which could be a reliable indicator of invasive tumors in small biopsies of superficial lesions. Another study showed that the presence of tissue eosinophilia particularly in close association with striated damaged muscle fibers is associated with advanced disease. Some studies suggested that tissue eosinophilia could be used as a predictive factor for lymph node metastases or locoregional recurrences. However, no significant association between tissue eosinophilia and survival outcomes was reported.
The biological role of tissue eosinophilia in SCC is still unclear and further studies are needed to clarify the prognostic role of eosinophilic infiltration in SCC.
Unfortunately, gingival SCCs are notorious for this endophytic growth pattern and are often discovered very late in the course of the disease when they explode onto the surface. The prognosis is very poor despite advances in treatment with the overall 5-year survival rate being about 50%. The mainstay of treatment is surgery with or without radiotherapy. However, there is significant morbidity from the surgery and radiation therapy as well. Early detection is critical to improve the outcome for these patients.
References
- Mascitti M, Togni L, Rubini C, Troiano G, Lo Muzio L, Santarelli A. Tumour-associated tissue eosinophilia (TATE) in oral squamous cell carcinoma: a comprehensive review. Histol Histopathol. 2021;36(2):113-122. doi:10.14670/HH-18-250
- Lowe D, Fletcher CD. Eosinophilia in squamous cell carcinoma of the oral cavity, external genitalia and anus–clinical correlations. Histopathology. 1984;8(4):627-632. doi:10.1111/j.1365-2559.1984.tb02375.x
- Falconieri G, Luna MA, Pizzolitto S, DeMaglio G, Angione V, Rocco M. Eosinophil-rich squamous carcinoma of the oral cavity: a study of 13 cases and delineation of a possible new microscopic entity. Ann Diagn Pathol. 2008;12(5):322-327. doi:10.1016/j.anndiagpath.2008.02.008
- Oliveira DT, Biassi TP, Faustino SE, Carvalho AL, Landman G, Kowalski LP. Eosinophils may predict occult lymph node metastasis in early oral cancer. Clin Oral Investig. 2012;16(6):1523-1528. doi:10.1007/s00784-011-0651-7
- Rakesh N, Devi Y, Majumdar K, Reddy SS, Agarwal K. Tumour associated tissue eosinophilia as a predictor of locoregional recurrence in oral squamous cell carcinoma. J Clin Exp Dent. 2015;7(1):e1-e6. Published 2015 Feb 1. doi:10.4317/jced.51610
Quiz Answers
Q1 = B. Squamous Cell Carcinoma
Q2 = True