A 30 year old patient presented with a pathologic mandible fracture and loose teeth following minimal trauma. CT imaging revealed a thin mandibular body and ramus with superimposed areas of permeative destruction and erosion, and a minimally displaced fracture of the mandibular angle. The ipsilateral maxillary sinus appeared hypoplastic. A segmental mandibulectomy with reconstruction was performed. The disease progressed within one year requiring total mandibulectomy and prosthetic replacement.
Q1. What is the diagnosis
Q2. What are the characteristic histologic features?
Gorham-Stout Disease.
Gorham-Stout Disease, also known vanishing bone disease or massive osteolysis, is a rare disorder that usually affects young adults but has a wide age range. It is considered to be an aggressive variant of hemangioma/lymphangioma, and is characterized by a proliferation of lymphatic spaces in bone resulting in osteolysis. The disease is named after Lemuel Whittington Gorham and Arthur Purdy Stout, who, in 1955, described the histologic features and established that the osteolysis was always associated with vascular proliferation. The proposed pathogenesis is a defect in lymphatic formation, either acquired or developmental, but the exact mechanism for osteolysis is not known. The etiology of Gorham-Stout disease remains unknown, and in fact whether it is a true neoplasm versus a reactive process is still debated.
Gorham-Stout disease can affect any bone, but usually affects the appendicular skeleton with predilection for the humerus, scapula, pelvis and skull. Involvement of the jaws is relatively uncommon, but the mandible is more commonly affected than the maxilla: A review of 185 cases reported in the literature from 1955 to 2013 reported that 27 cases showed involvement of the mandible, 7 showed involvement of the maxilla, and 4 showed involvement of both mandible and maxilla.
Radiographically, the earliest finding can be small intramedullary or subcortical radiolucent foci. As the disease progresses partial or complete dissolution of a bone or several adjacent bones is evidenced. This often occurs in a concentric pattern causing a “licked candy stick” or “mouse tail” appearance. Usually there is no solid or expansile mass lesion, and the disease can cross joints.
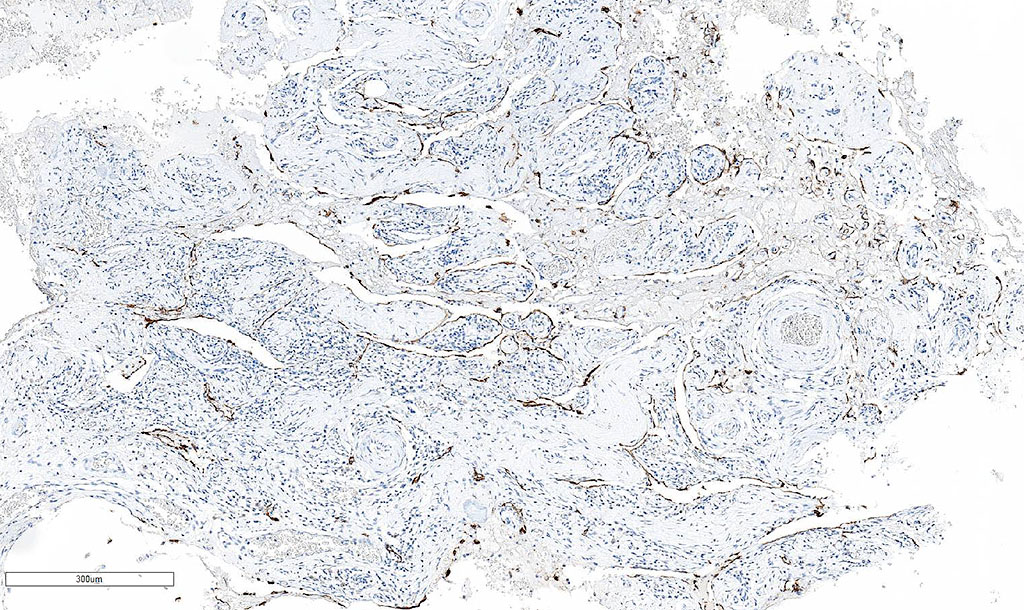
Histologically, the affected bones show a benign vascular proliferation composed of dilated, thin-walled blood vessels and/or lymphatics, sometimes resembling a hemangioma. Lymphatic vessels are not present in normal bones, but are present in medullary and cortical regions of bones in patients with Gorham-Stout Disease and may be a subtle finding early in the disease, especially because the surrounding bone shows minimal to no osteoblastic response. As the disease progresses, bone is subsequently replaced by variable amount of fibrous tissue with increased vascularity. Osteoclastic activity may be seen at the leading edge. The vascular walls may be difficult to appreciate in fragmented specimens, and in those scenarios, immunohistochemistry can be performed to highlight the characteristic lymphatic vessel proliferation with lymphatic markers such as D2-40 (see image), CD34, CD31, ERG, and FLI-1 and Factor VIII. As the histologic features are not specific, the diagnosis requires careful correlation with radiographic findings and the clinical features.
The disease may spontaneously arrest and stabilize, but often progresses rapidly and causes disability. There is no known optimal therapy, but surgical resection and localized radiation have been used when feasible. The role of systemic therapy has not been systematically studied.
References
- Gorham LW, Stout AP. Massive osteolysis (acute spontaneous absorption of bone, phantom bone, disappearing bone); its relation to hemangiomatosis. J Bone Joint Surg Am 1955;37-A:985-1004.
- Stocker, JT, Dehner, LP, and Husain, AN (2012). Stocker and Dehner’s pediatric pathology: Fourth edition. Wolters Kluwer Health Adis (ESP).
- Fletcher CD (2013). Diagnostic histopathology of tumors: Fifth edition. Elsevier Health Sciences.
- Nielsen, GP, Rosenberg, AE, Deshpande, V, Hornicek, FJ, Kattapuram, SV, Rosenthal, DI (2017). Diagnostic Pathology: Bone, second edition. Elsevier Health Sciences.
- Edwards JR, Williams K, Kindblom LG, Meis-Kindblom JM, Hogendoorn PC, Hughes D, Forsyth RG, Jackson D, and Athanasou NA. Lymphatics and bone. Hum Pathol. 2008 Jan;39(1):49-55.
- Dellinger MT, Garg N, and Olsen BR. Viewpoints on vessels and vanishing bones in Gorham–Stout disease. Bone. 2014 Jun; 63:47-52.
Quiz Answers
Q1 = B. Gorham-Stout disease
Q2 = B. Benign lymphatic or vascular proliferation and osteolysis