Head & Neck Case Review
October, 2021
History
An adult woman with a significant smoking history presented to the emergency department with chronic unilateral otalgia and worsening odynophagia causing decreased appetite and weight loss. The patient denied fevers or B symptoms. Physical exam demonstrated a firm, exophytic, non-ulcerated mass in the palatine tonsil. CT scan showed a tonsillar mass with bilateral lymphadenopathy throughout the neck. The patient underwent bilateral tonsillectomy.
Images
Quiz
Q1. What is the diagnosis?
- A. Extramedullary plasmacytoma
- B. Systemic lupus erythematosus
- C. T. pallidum infection
- D. Granulomatosis with polyangiitis
Q2. What is the most specific confirmatory test?
- A. c-ANCA
- B. Flow cytometry, serum protein electrophoresis and bone marrow biopsy
- C. Direct immunofluorescence
- D. Serum RPR and VDRL
- E. Serum RPR and FTA-ABS
Diagnosis
Oropharyngeal syphilis
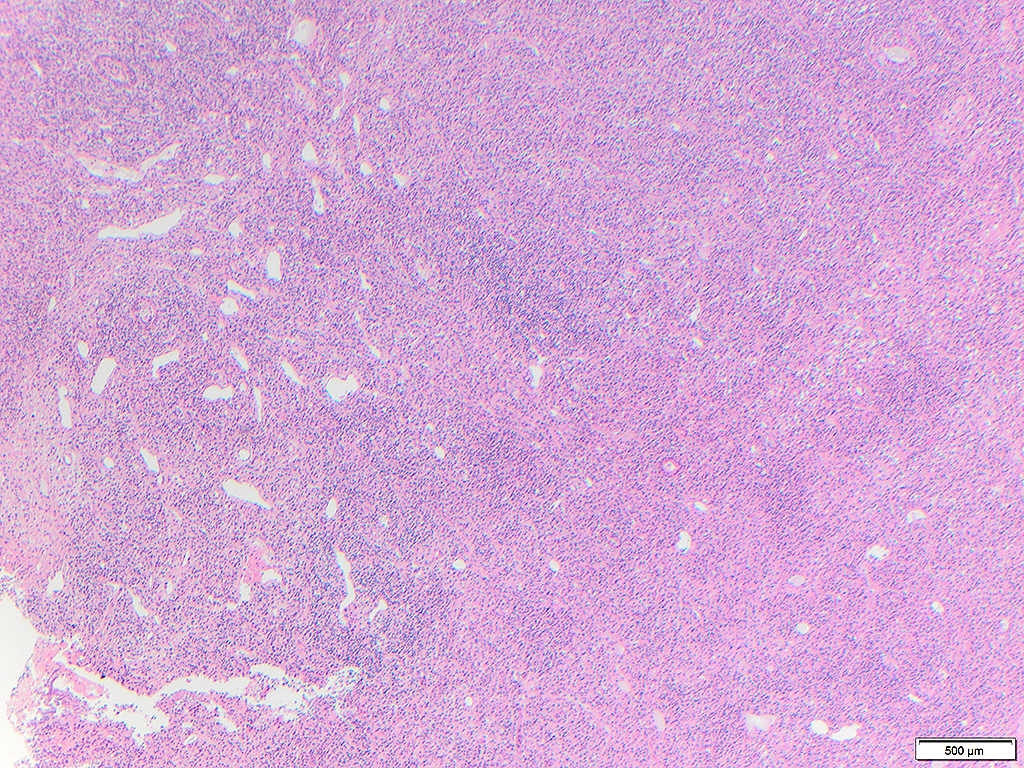
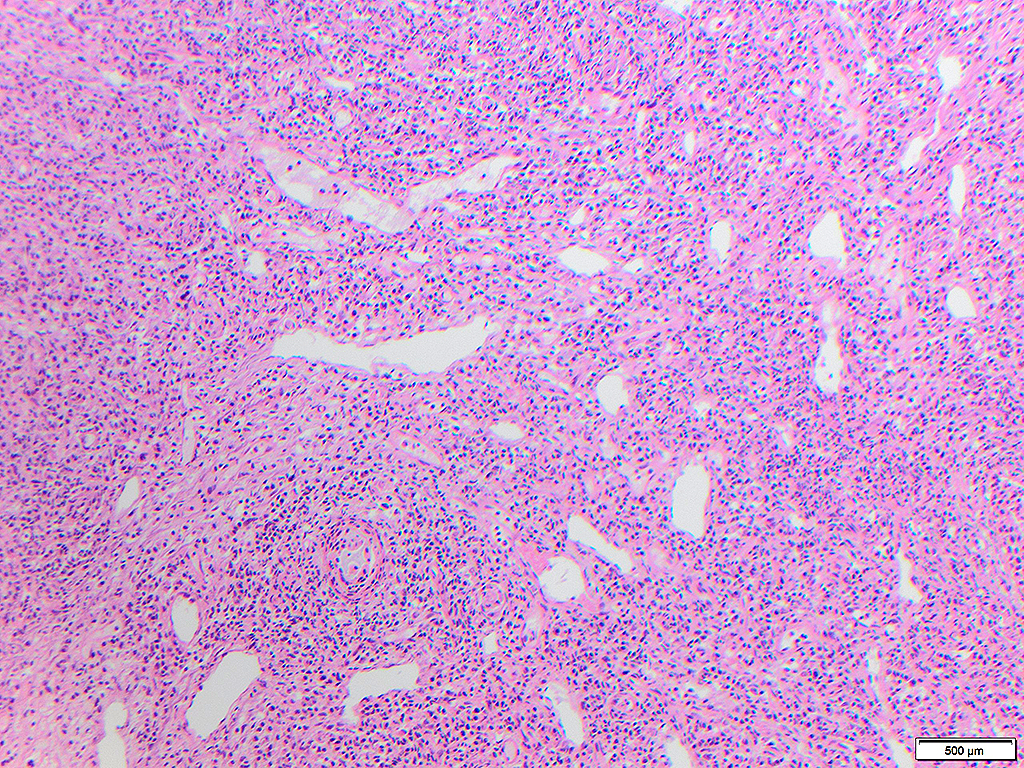
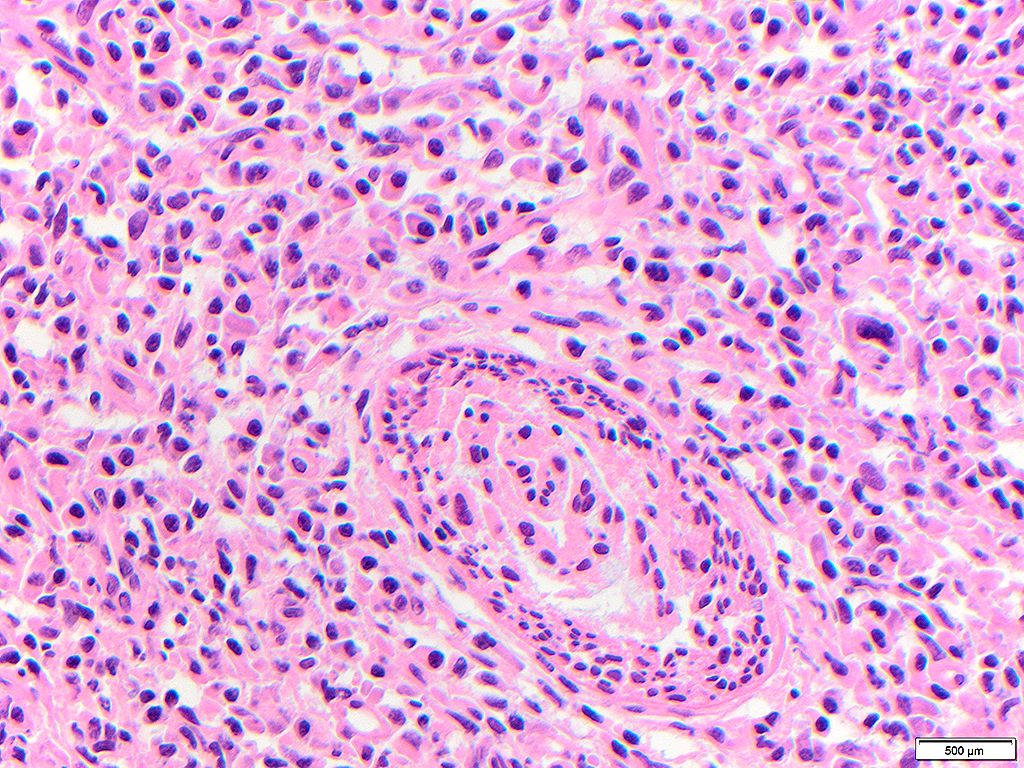
Syphilis is a sexually transmitted infection caused by the bacteria Treponema pallidum. In general, the histologic features of syphilis are dense chronic inflammatory infiltrates composed mostly by lymphocytes and plasma cells with vague perivascular accentuation. Syphilitic oral ulcers with only acute inflammation devoid of lymphoplasmacytic infiltrate have been reported. Other findings may include effacement of the normal architecture of the involved organ, swollen endothelial cells, and occlusive endovasculitis (luetic vasculitis). Lymph nodes may show a marked follicular hyperplasia, thickened capsule, fibrosis, necrosis, and/or multinucleated giant cells. The morphologic differential diagnosis is broad and includes other infections (bacterial, fungal and viral), trauma, neoplasms, auto-immune disorders, and allergies. In lymph nodes, the morphologic differential diagnosis includes reactive hyperplasia, granulomatous diseases such as tuberculosis, sarcoidosis, cat scratch disease, and even follicular lymphoma because of marked reactive follicular hyperplasia.
Reports of involvement of oral cavity and oropharynx are rare in the pathology literature. A recent case series by Deng et al (1) described three cases of oral cavity involvement, one of which also showed oropharyngeal involvement. Most chancres occur in the anogenital region, but the oral cavity and lips are not uncommon extragenital sites. In the oral cavity, primary syphilis usually presents in the form of a painless non-healing ulcer. The classic presentation for secondary syphilis in the oral cavity consist of multiple white mucous patches, with condyloma lata and split papules also reported.
Hamlyn et al (5) reported 3 cases of secondary syphilis presenting as tonsillitis in Australia in 2006, one of which had a tonsillectomy showing reactive follicular hyperplasia with increased plasma cells. In the present case, there was complete effacement of tonsil architecture without recognizable crypts in both tonsils with pseudotumor in one tonsil. Vascular accentuation of the infiltrates and edematous endothelial cells were important morphologic clues to the diagnosis. Because the tonsils are specialized mucosa, morphologic features may include those described in lymph nodes.
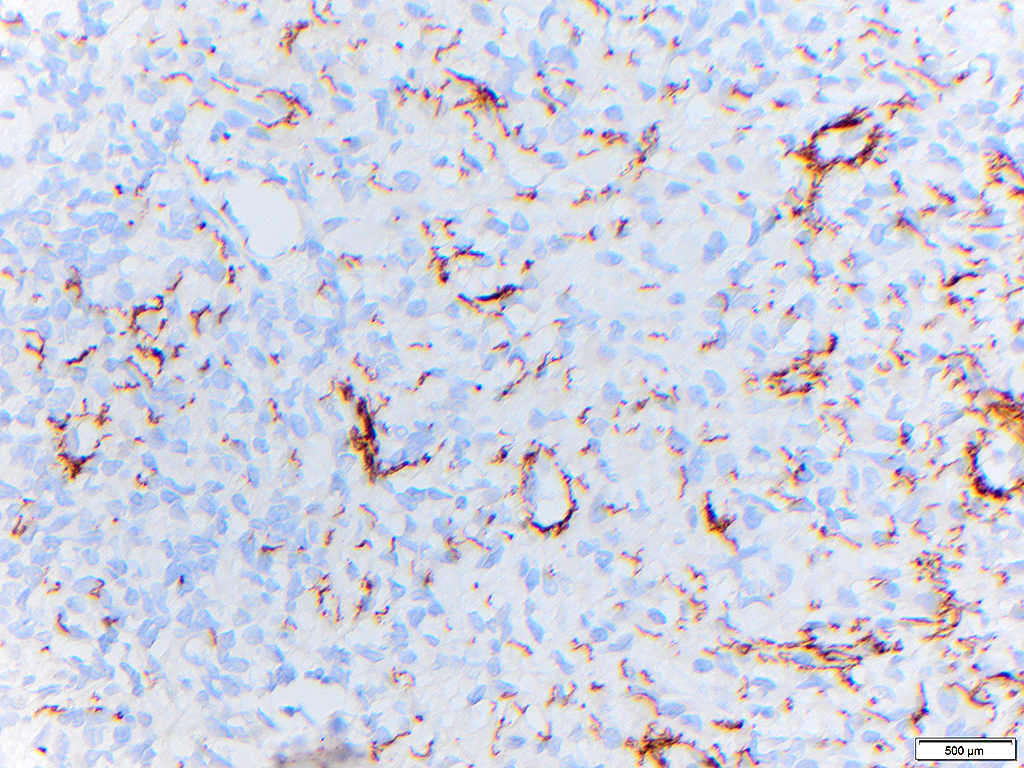
The presence of the spirochete can be demonstrated by immunohistochemistry which will highlight corkscrew shaped organisms and may show perivascular aggregates of the organisms, as in this case. Most laboratories use an antibody that is highly specific for T. pallidum, but confirmation with serology is generally recommended (discussed below). Special staining with Warthin-Starry stain is a less specific alternative when immunohistochemistry is not available.
Transmission occurs person to person by direct contact with a chancre. Despite well-documented prevention methods and treatment, the incidence rates has been steadily increasing throughout the United States since the year 2000, with a steady increase involving many population groups. Untreated syphilis is potentially life-threatening with consequences that include neurological complications, hearing loss, and blindness.
Based on the duration of the infection, syphilis can be classified as primary, secondary, tertiary, and latent. Primary syphilis typically presents as a painless ulceration at the site of inoculation, usually solitary, and associated to localized lymphadenopathy that develops within 3 weeks of the exposure. Secondary syphilis usually occurs within 2 to 8 weeks from exposure and is characterized by skin rashes and mucous lesions, however the presentation can be even more nonspecific with symptoms such as, fever, pain and disseminated lymphadenopathy. The tertiary stage occurs within 10 to 30 years of the infection, and symptoms vary according the affected organs (any organ can be affected).
T. pallidum cannot be cultured in the clinical microbiology laboratory, therefore serologic tests are generally necessary for the diagnosis of the disease in any stage. A reactive treponemal test (FTA-ABS) in addition to a reactive nontreponemal test (RPR) is highly specific for infection. Treponemal tests may remain reactive indefinitely, and are not useful for monitoring therapy. Nontreponemal tests include RPR and VDRL. These tests detect IgM and IgG anti-cardiolipin antibody, produced in response to host cell damage and cardiolipins released from treponemes, which can lead to false positive tests in the presence of other anti-cardiolipin antibody producing conditions. In addition, RPR titers are negative or low early in primary syphilis, can become negative after several years, even without therapy and titers drop rapidly after treatment of primary or secondary syphilis. All positive nontreponemal tests must be confirmed by a treponemal test to detect antibodies against the T. pallidum, such as FTA-ABS, that remains reactive, irrespective of treatment, for increased specificity.
To date, the treatment of choice is still penicillin as no resistance of the Treponema pallidum has been observed against this antibiotic. The dosage varies according the stage of the disease. In the United States syphilis is listed in the National Notifiable Diseases Surveillance System (NNDSS) of the Centers for Disease Control, and all cases of probable and confirmed syphilis meeting the CDC case definitions should be reported.
The clinical diagnosis of syphilis can be challenging because of the many different presentations. Similarly, the histopathology of syphilis is characterized by nonspecific features that can mimic other disorders. As a consequence, a high index of suspicion is required for the diagnosis. Multi-institutional collaboration studies may be useful to describe specific histopathologic characteristics of primary or secondary syphilis occurring in specialized mucosae of the oropharynx.
References
- Deng F, Thompson LDR, Lai J. Unexpected Reason for Non-healing Oral Ulcers: Syphilis. Head Neck Pathol. 2021 Aug 3. doi: 10.1007/s12105-021-01348-y. Epub ahead of print. PMID: 34342809.
- Thompson LDR. Oral Syphilis. Ear Nose Throat J. 2021 Sep;100(5_suppl):538S-539S. doi: 10.1177/0145561319890154. Epub 2019 Nov 24. PMID: 31760793.
- Schmidt R, Carson PJ, Jansen RJ. Resurgence of Syphilis in the United States: An Assessment of Contributing Factors. Infect Dis (Auckl). 2019;12:1178633719883282. Published 2019 Oct 16. doi:10.1177/1178633719883282
- Komeno Y, Ota Y, Koibuchi T, Imai Y, Iihara K, Ryu T. Secondary Syphilis with Tonsillar and Cervical Lymphadenopathy and a Pulmonary Lesion Mimicking Malignant Lymphoma. Am J Case Rep. 2018 Mar 4;19:238-243. doi: 10.12659/ajcr.907127. PMID: 29502129; PMCID: PMC5846205.
- Hamlyn E, Marriott D, Gallagher RM. Secondary syphilis presenting as tonsillitis in three patients. J Laryngol Otol. 2006 Jul;120(7):602-4. doi: 10.1017/S002221510600096X. Epub 2006 Mar 24. PMID: 16556350.
- Yuan Y, Zhang X, Xu N, et al. Clinical and pathologic diagnosis and different diagnosis of syphilis cervical lymphadenitis. Int J Clin Exp Pathol. 2015;8(10):13635-13638. Published 2015 Oct 1.
- ClinLab Navigator [http://www.clinlabnavigator.com/syphilis-serology.html]. Accessed September 2021
Quiz Answers
Q1 = C. T. pallidum infection
Q2 = E. Serum RPR and FTA-ABS
Contributors
Igor Damasceno Vidal, MD, PGY-2 resident
Pathology Residency Program
University of Alabama at Birmingham School of Medicine
Manuel Lora Gonzalez, MD, Assistant Professor
Department of Pathology
University of Alabama at Birmingham Hospital & School of Medicine