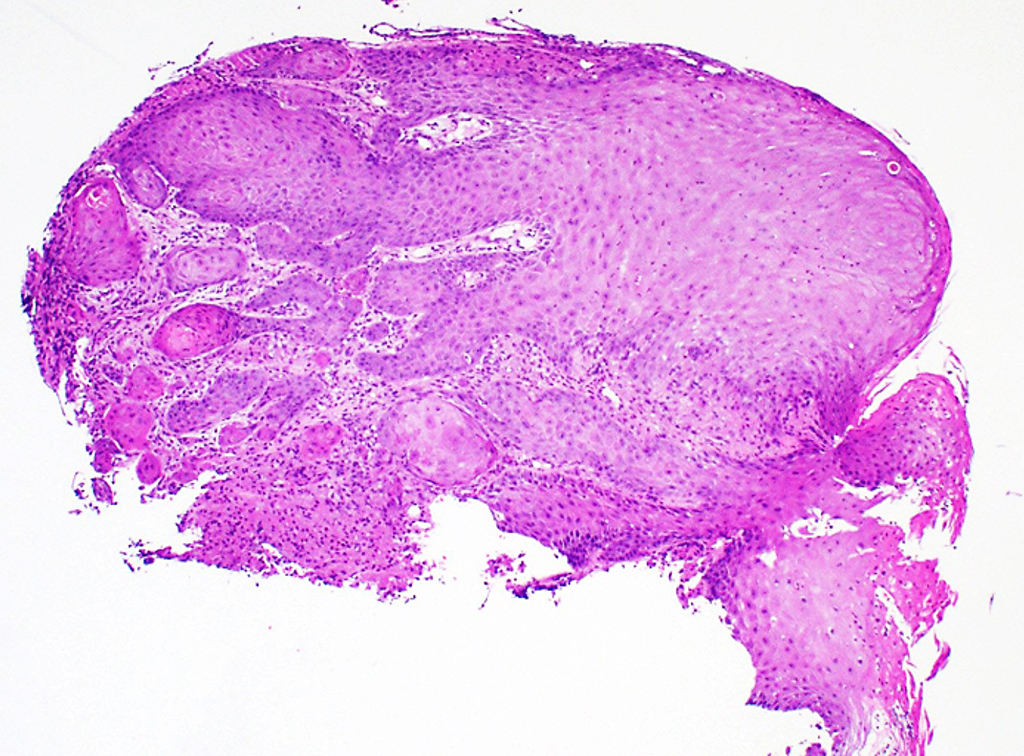
A 50-year-old man presents with a 6-month history of a left tongue lesion which was biopsied. Characteristic H&E stained sections and one immunostain are shown.
Q1. Which of the following is true regarding this lesion?
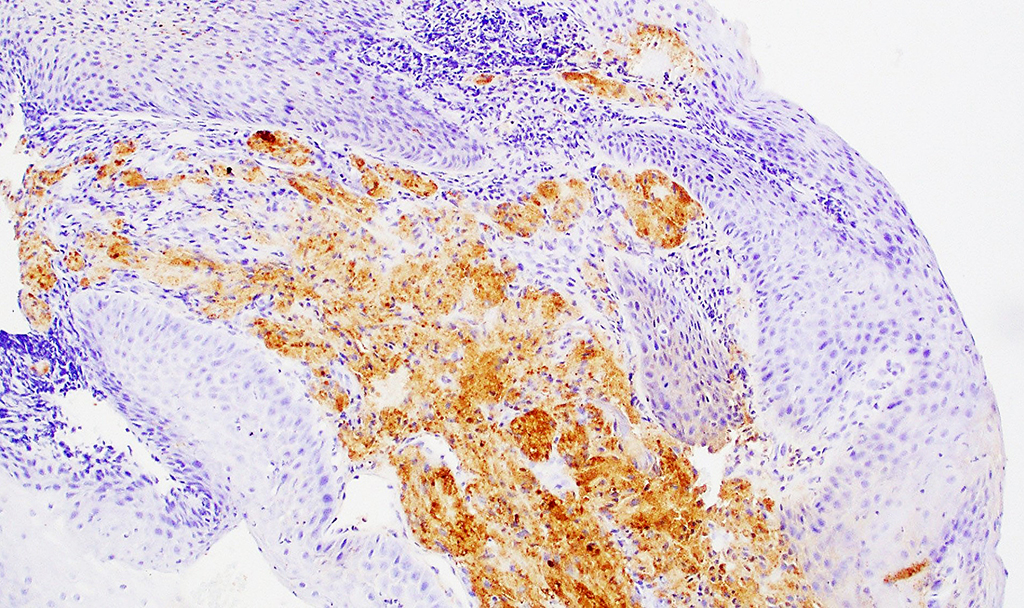
Q2. Which immunohistochemical stain is used to help diagnose this lesion and is shown here?
Granular cell tumor with pseudoepitheliomatous hyperplasia
Granular cell tumor (GCT) is a relatively uncommon lesion of Schwann cell differentiation which can affect any anatomic location. The most frequently-affected region is the head and neck, with the highest prevalence in the tongue. It typically arises in the third to the sixth decades and has a slight female preponderance.
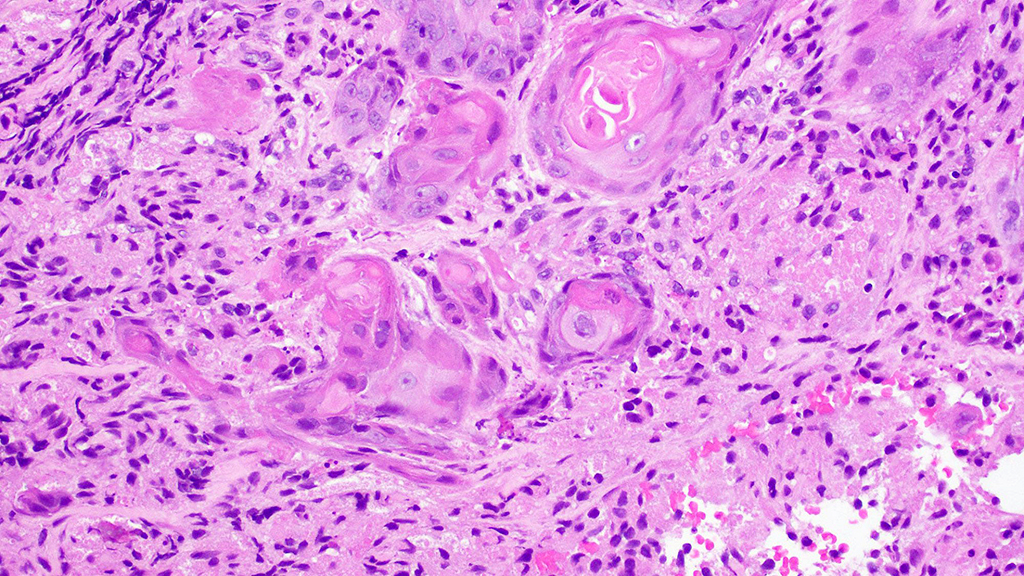
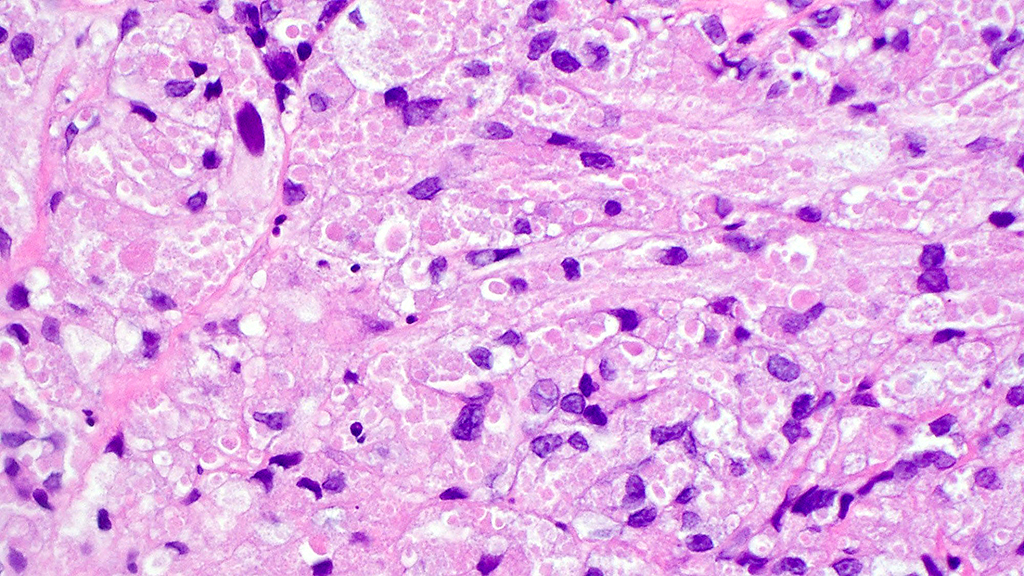
A properly oriented H&E–stained section is very important for diagnostic interpretation. Histologically, GCT is characterized by an ill-defined tumor, composed of plump polygonal cells with small nuclei and abundant eosinophilic granular cytoplasm. Pseudoepitheliomatous hyperplasia (PEH) occurs in up to 50% of granular cell tumors – typically in the overlying epithelium – and often mimics invasive squamous cell carcinoma (SCC), although there have been rare reports of the coexistence of PEH and invasive SCC. The exact explanation for the association between GCT and PEH is unknown but is postulated to be due to the proliferative activity of basal cells that interact with granular cells and neighboring epithelial cells.
PEH is a reactive epithelial proliferation found in association with several neoplastic and reactive processes. Histologically, it is seen as cords and strands of squamous epithelium that extends to the underlying dermis or submucosa and that displays a pseudo-infiltrative pattern of growth which can closely mimic invasive squamous cell carcinoma. PEH can rarely be found in association with basal cell carcinoma (BCC) but the epidermal hyperplasia has a follicular differentiation and is often eccentric relative to the BCC rather than directly overlying it. Differentiating PEH from invasive SCC especially on superficial and limited biopsies can be extremely challenging. SCC is favored by more pronounced cytologic atypia and other features of malignancy such as nuclear pleomorphism, increased mitotic activity (especially presence of atypical mitoses), and perineural/lymphovascular invasion. When classic cytologic signs of malignancy are lacking, PEH clinical findings and/or the presence of an underlying reason for the presence of PEH tilt the diagnostic probability in favor of PEH.
By immunohistochemistry, the tumor cells are positive for S100 (cytoplasmic and nuclear staining as shown in the image), SOX10 (nuclear), inhibin, and calretinin. The cytoplasmic eosinophilic granules (phagolysosomes) are PAS positive, diastase resistant, and are also often highlighted by CD68.
GCT is usually a benign tumor. Histologic criteria for malignant GCT is still a topic of debate. GCTs with nuclear pleomorphism, high N:C ratio, prominent nucleoli, spindle cell morphology, necrosis, and increased mitotic activity >2/10 are considered malignant. The optimal treatment for GCT is complete surgical excision as they are not sensitive to radiotherapy or chemotherapy.
References
- Mobarki M, Dumollard JM, Dal Col P, Camy F, Peoc’h M, Karpathiou G. Granular cell tumor a study of 42 cases and systemic review of the literature. Pathol Res Pract. 2020 Apr;216(4):152865. doi: 10.1016/j.prp.2020.152865. Epub 2020 Feb 12. PMID: 32089415.
- Caroppo, Danila, et al. “Coexistent Squamous Cell Carcinoma and Granular Cell Tumor of Head and Neck Region: Report of Two Very Rare Cases and Review of the Literature.” International Journal of Surgical Pathology, vol. 26, no. 1, 7 Aug. 2017, pp. 47–51.
- Elena Zarovnaya and Candice Black. Distinguishing Pseudoepitheliomatous Hyperplasia from Squamous Cell Carcinoma in Mucosal Biopsy Specimens from the Head and Neck. Archives of Pathology & Laboratory Medicine: August 2005, Vol. 129, No. 8, pp. 1032-1036.
- Nayak, Vaidhehi Narayan, et al. “Pseudoepitheliomatous Hyperplasia in Oral Lesions: A Review.” Journal of International Oral Health: JIOH, vol. 7, no. 9, 2015, pp. 148–52.
Quiz Answers
Q1 = B. The lesional cells are filled with PAS+, diastase resistant granules
Q2 = C. S100