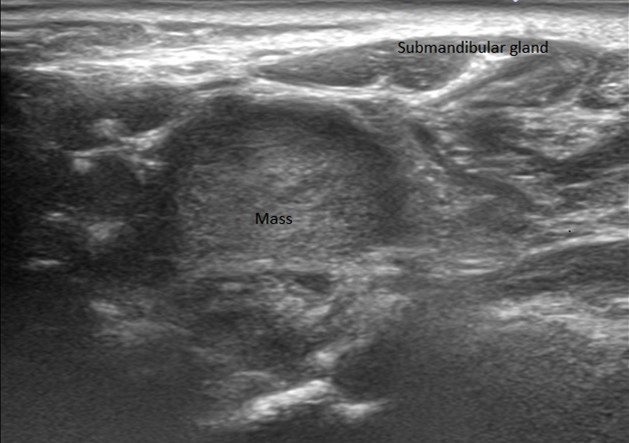
A 72-year-old female presents with hoarseness of voice and dysphagia. A 3.2 x 1.9 x 2.7 cm heterogenous nodule in the left neck adjacent to the submandibular gland is noted on ultrasound. An ultrasound guided core needle biopsy is performed.
1. Which of the following is TRUE?
2. TRUE or FALSE: 10% of these tumors are familial/inherited.
Head and neck (parasympathetic) paraganglioma with sclerosis
Head and neck paragangliomas are neuroendocrine tumors that typically arise from parasympathetic ganglia in the head and neck region. They show a female predilection and appear to be driven by chronic hypoxia as evidenced by a higher prevalence in populations living at higher altitudes. The most common head and neck site is the carotid body (60%), followed by the middle ear (i.e. jugulotympanic, 30%), vagus nerve (10%), larynx (<1%), and thyroid (rare reports).
Head and neck paragangliomas are most often clinically non-functional and typically present as asymptomatic, often palpable masses, but vagal tumors may rarely (<1%) secrete catecholamines. Jugulotympanic tumors characteristically present with pulsatile tinnitus, while laryngeal paragangliomas may be accompanied by hoarseness. Carotid body tumors classically demonstrate horizontal mobility on palpation but vertical fixation (Fontaine sign), presumably due to their close association with the carotid artery.
Preoperative core needle and fine needle aspirate biopsies are typically not indicated for head and neck paragangliomas and should in fact be avoided when suspected clinically or radiologically, since these procedures pose rare but significant dangers given their vascularity and proximity to vital structures such as the carotid artery.
When resected, paragangliomas grossly show an ovoid or fusiform appearance and may be variably adherent to adjacent structures. Jugulotympanic tumors are notably ill-defined and may show bone and cavernous sinus invasion. Cut surfaces are highly vascular and may range from a homogeneous tan/brown to a more fibrous white. Prior infarction/embolization may impart a more variegated appearance.
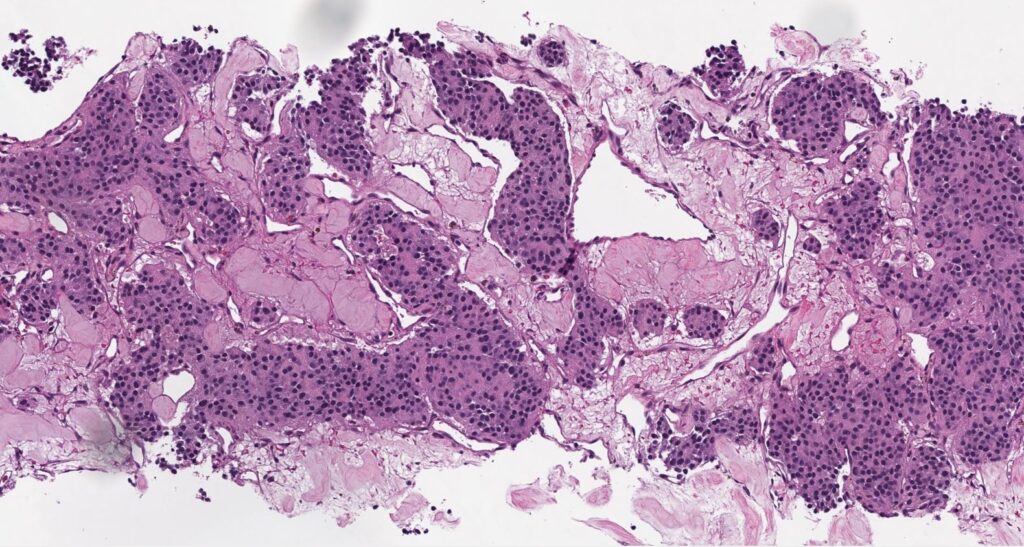
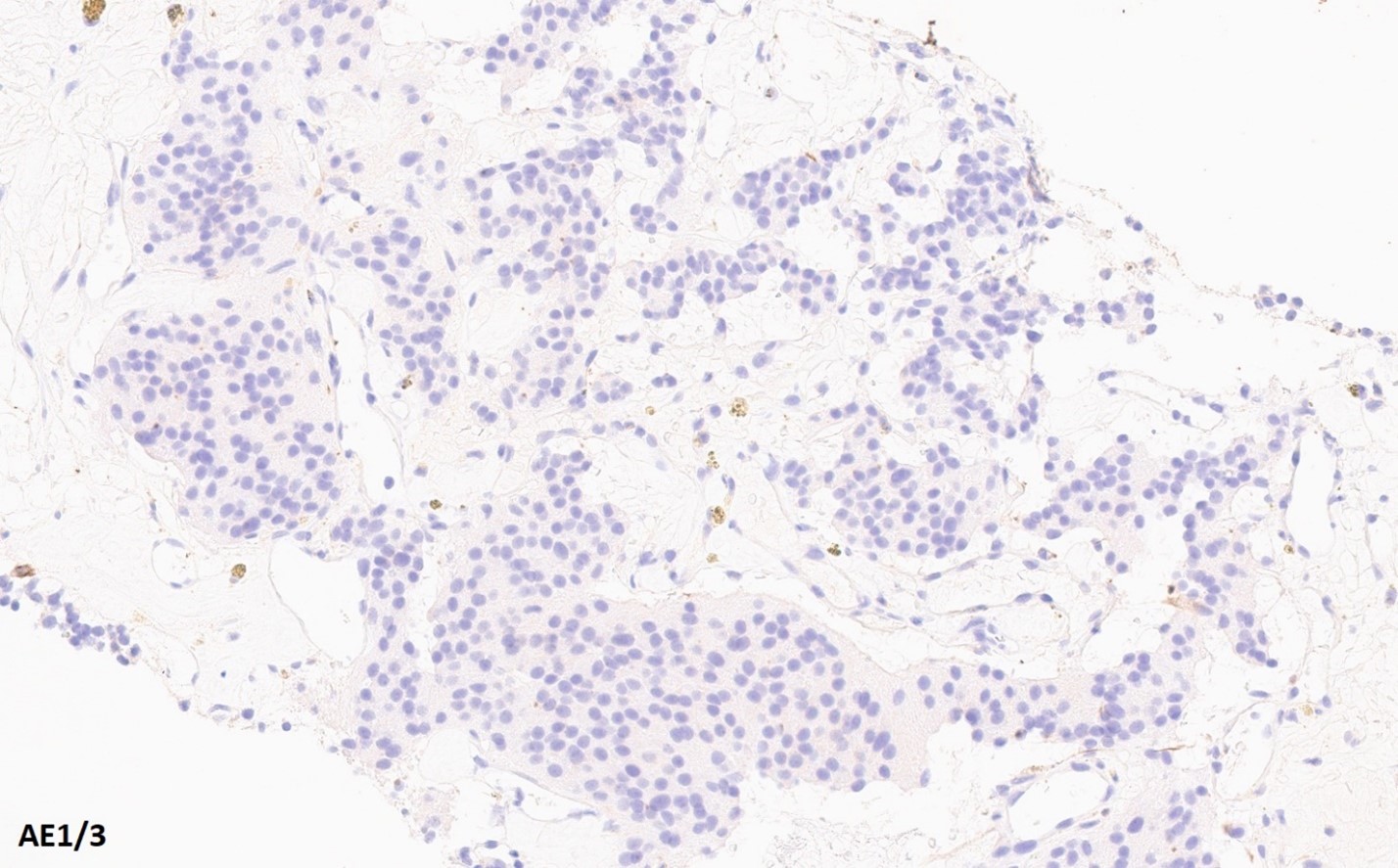
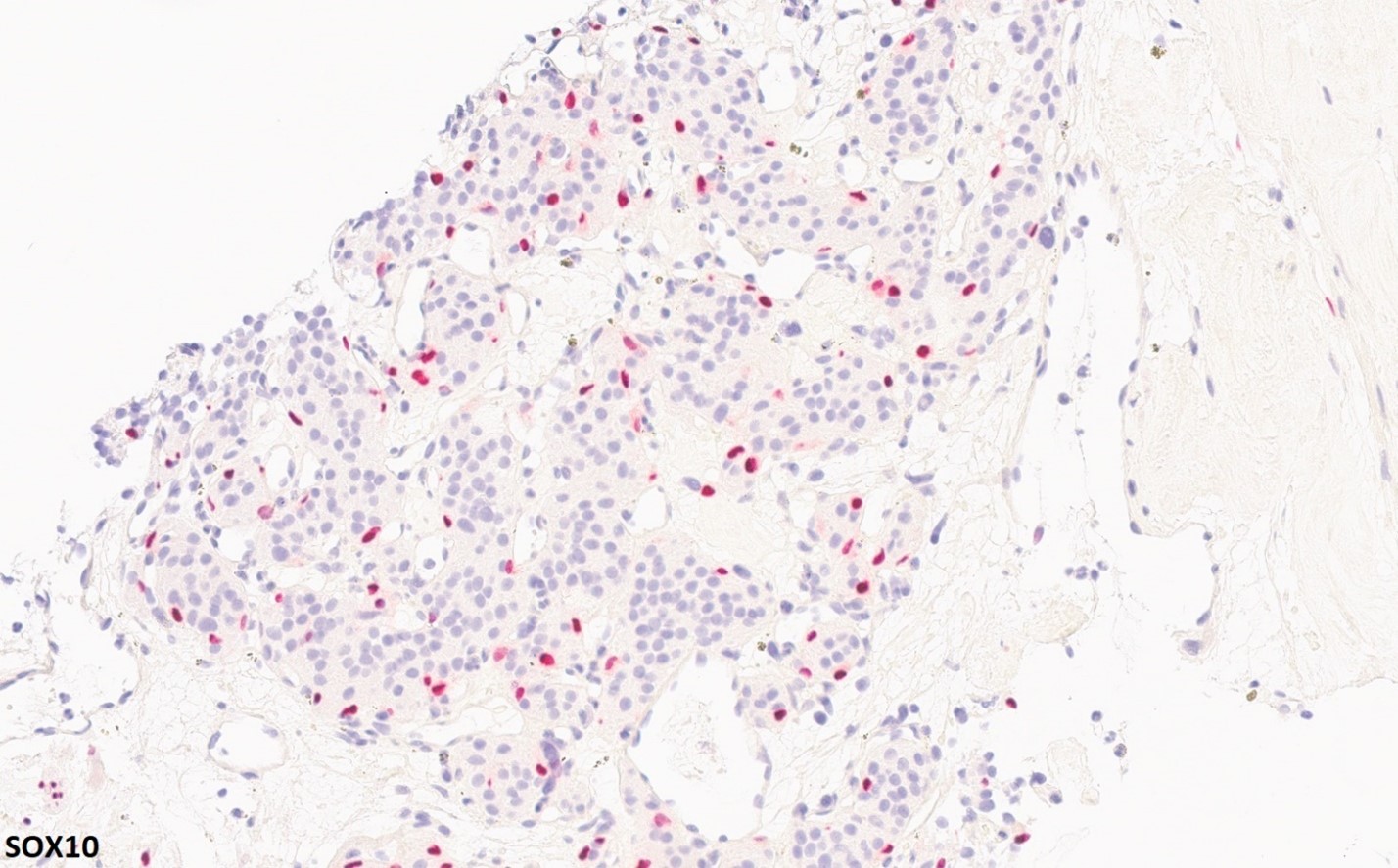
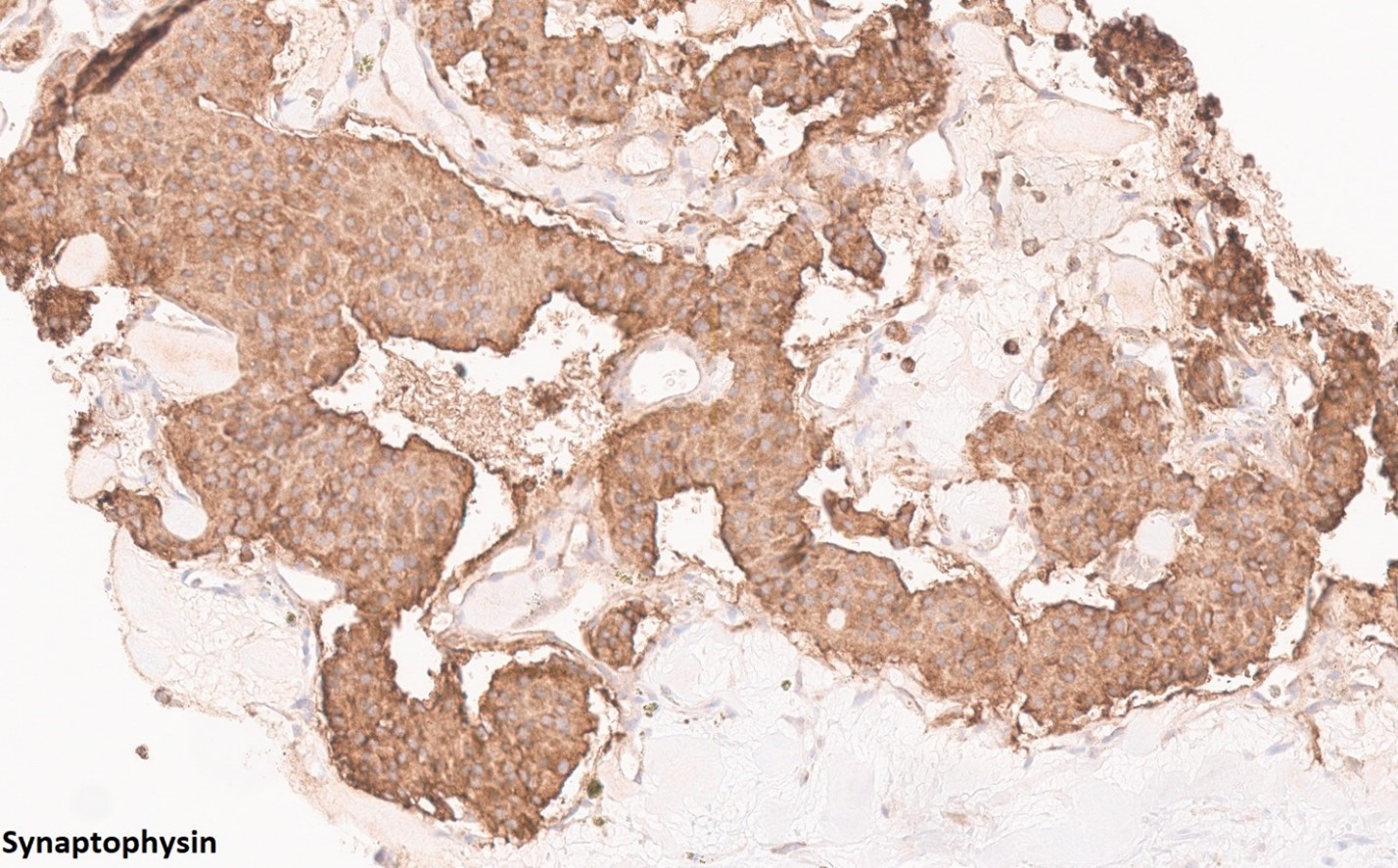
Histologically, paragangliomas are well-demarcated but often uncircumscribed, and may infiltrate adjacent tissues. The classic growth pattern consists of organoid (Zellballen) cellular nests composed of chief cells with a granular amphophilic or eosinophilic cytoplasm surrounded by a thin layer of spindled sustentacular cells and embedded in a highly vascular stroma. The nuclei show a “salt-and-pepper” type chromatin as well as random nuclear size variation typical of many neuroendocrine tumors. Tumor cells are characteristically positive for neuroendocrine markers such as INSM1, synaptophysin, and chromogranin, but almost invariably negative for cytokeratins. Notably, GATA3 expression may be variably expressed in paragangliomas. Sustentacular cells are highlighted by S100 or SOX-10. Head and neck paragangliomas, especially those of the carotid body, are prone to considerable sclerosis which then imparts a corded “pseudoinfiltrative” appearance.
The morphologic differential diagnosis for head and neck paragangliomas can be broad if not suspected initially and encompasses primary clear cell or oncocytic lesions of thyroid, parathyroid, and salivary glands. Vascular metastases such as renal cell carcinoma or melanoma and even nested epithelioid sarcomas such as alveolar soft part sarcoma (historically miscategorized as ‘non-chromaffin paraganglioma’) could also be considered. The immunophenotype above also helps to resolve most of these considerations. Key immunohistochemical pitfalls include GATA3 reactivity in parathyroid lesions. However, parathyroid lesions are expected to express cytokeratins and tend to be more strongly positive for GATA3 than head and neck paragangliomas. Another key pitfall is the occasional presence of S100 positive sustentacular-like cells in neuroendocrine neoplasms/carcinomas. However, aside from the greater heterogeneity in growth patterns, neuroendocrine neoplasms/carcinomas are expected to express cytokeratins. Medullary thyroid carcinoma and hyalinizing trabecular tumor of thyroid can be delineated by TTF-1 and PAX-8 reactivity, in addition to expression of keratins and usually absent sustentacular cell populations. Hyalinizing trabecular tumor (historically known as paraganglioma-like adenoma of thyroid) is also known to harbor PAX8::GLIS3 or GLIS1 rearrangements.
The “rule of 10’s” as applied to head and neck paragangliomas essentially falls flat. Key deviations from this include malignant potential and hereditary disposition.
Head and neck paragangliomas have low metastatic potential (4-6%), though this varies by subsite. Vagal paragangliomas have the highest metastatic potential (~15%), and jugulotympanic paragangliomas having the lowest (2%). Histologic features such as increased mitotic activity, necrosis, spindling, loss of sustentacular staining, and lymphovascular invasion are not reliably predictive of metastatic potential.
In contrast, they have a strong hereditary disposition (40-85% in some series). Most have mutations involving the succinate dehydrogenase complex. In contrast to pheochromocytomas, the prevalence of VHL, RET, or NF1 mutations is low. As the majority of succinate dehydrogenase complex alterations affects the succinate dehydrogenase B subunit, loss of SDHB immunostaining can be used as a screening tool to inform subsequent genetic testing.
References
- Hoang, V. T., et al. (2019). “Carotid body tumor: a case report and literature review.” J Radiol Case Rep 13(8): 19-30.
- WHO Classification of Tumours Editorial Board. Head and neck tumours. Lyon (France): International Agency for Research on Cancer; 2022. (WHO classification of tumours series, 5th ed.; vol. 9)
- Williams, M. D. (2017). “Paragangliomas of the Head and Neck: An Overview from Diagnosis to Genetics.” Head Neck Pathol 11(3): 278-287.
- Ordóñez NG, Ro JY, Mackay B. Alveolar soft part sarcoma. An ultrastructural and immunocytochemical investigation of its histogenesis. Cancer. 1989 May 1;63(9):1721-36. PMID: 2649226.
Quiz Answers
Q1 = B. These tumors are typically driven by mutations in the succinate dehydrogenase complex.
Q2 = False.
Raja R. Seethala, MD
Professor of Pathology and Otolaryngology
University of Pittsburgh Medical Center