The patient is a 57 year-old male with a history of recurrent nephrolithiasis for 20 years. Serum biochemistry revealed: PTH 11.5 pmol/L (reference range, 2.0 – 9.3 pmol/L) and calcium 2.62 (reference range 2.20 – 2.60 mmol/L). A diagnosis of primary hyperparathyroidism was made. Pre-operative localizing studies were not helpful in determining location of a parathyroid lesion. Bilateral neck exploration was undertaken with planned parathyroidectomy.
Intraoperative findings included: three normal-appearing parathyroid glands (which were biopsied) and a single markedly enlarged left superior parathyroid gland (which was easily resected without adhesions). Intraoperative post-resection serum biochemistry revealed: PTH 3.4 pmol/L.
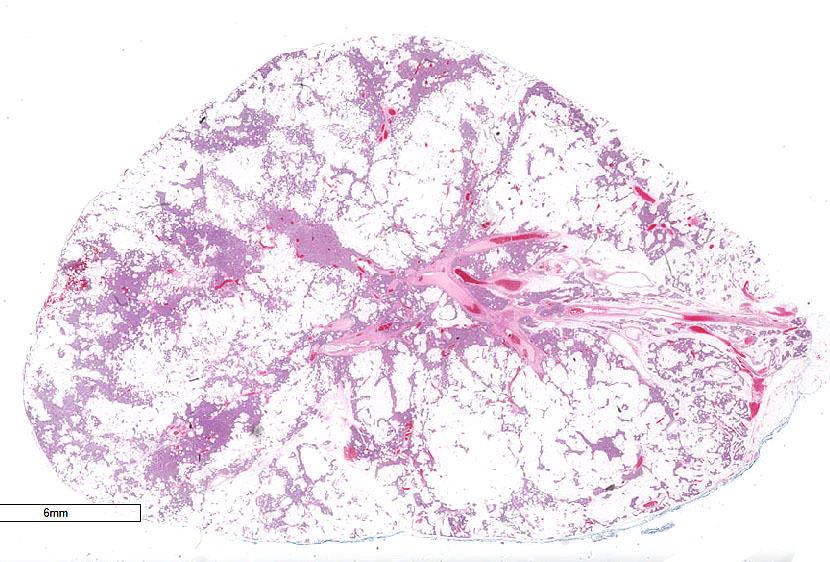
Surgical pathology received biopsies of the three grossly “normal-appearing” parathyroid glands which showed normocellular parathyroid tissue on histology (not pictured). The excised parathyroid weighed 4.27 g (fresh) and measured 3.1 cm in greatest dimension (pictured).
Q1. Compared to a conventional parathyroid adenoma, the entity in this case
Q2. The amount of adipose tissue is directly proportional to the body mass index of this patient.
Parathyroid Lipoadenoma.
Parathyroid lipoadenomas are a rare manifestation of primary hyperparathyroidism. Only a few sporadic cases have been described in the literature. To diagnose this entity, several factors must be considered, both clinical and histological. From the clinical perspective, evidence of primary hyperparathyroidism must exist, typically confirmed preoperatively via serum biochemistry (as in this case), as well as intraoperatively by single gland enlargement. In this case, the other three parathyroid glands were sampled and were appropriately normocellular. Moreover, a post-operative biochemical cure is supportive of the diagnosis.
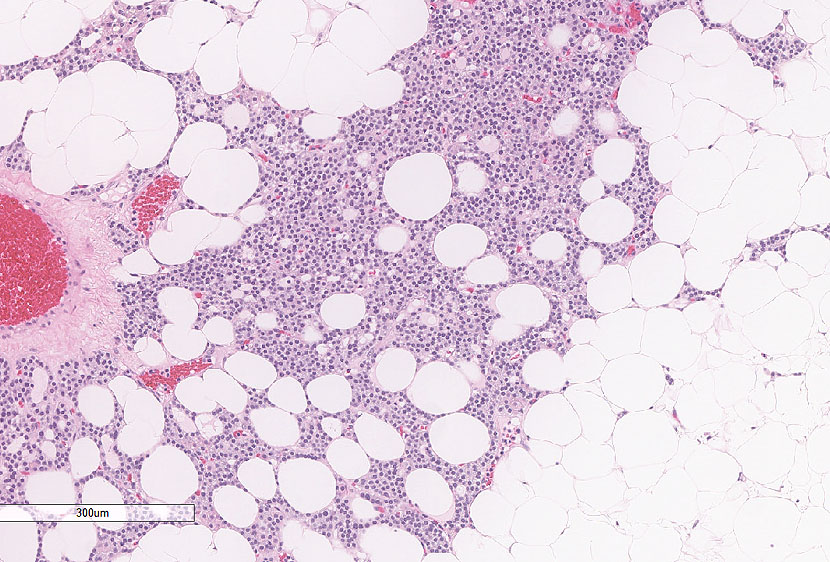
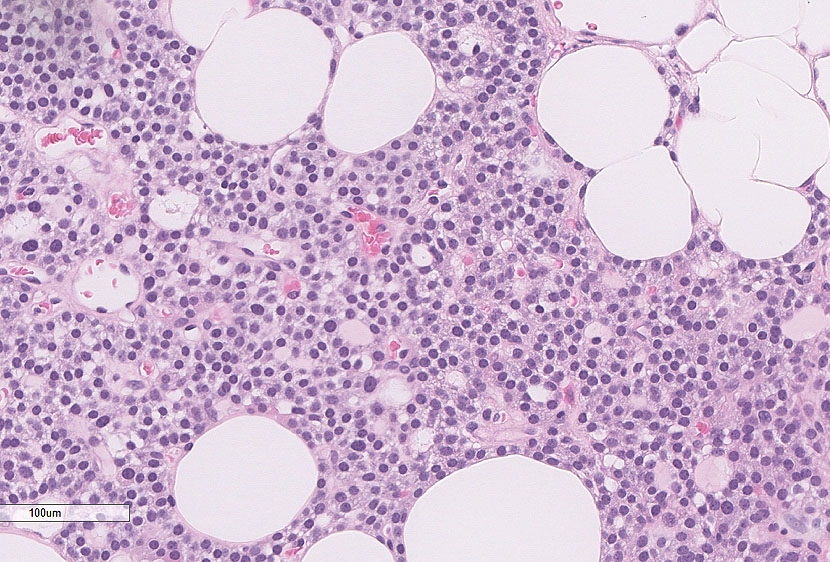
Histologically, parathyroid lipoadenoma exhibits extensive stromal adipose tissue and small, labyrinth-like nests of parathyroid cells, most often chief cells, arranged in cords or acini. Features of malignancy (invasion) and other atypical features (e.g. necrosis, increased mitotic count, fibrous bands) should be absent. Of note, there is no set definition or proportion of adipose tissue required for a diagnosis of lipoadenoma. However, many use >50% as a rough guide. Importantly, parathyroid glands are normally adipose-rich (~ 50% parenchyma / 50% fat). Assessing only the ratio of parenchymal cells to adipocytes is not necessarily reliable in the diagnostic evaluation of parathyroid disease. Size and weight are also important in defining an abnormal gland, and intraoperative and postoperative biochemical workup distinguishes uniglandular disease (adenoma) from multiglandular disease (hyperplasia).
Recognizing lipoadenoma is important for two reasons: (1) not to mistake it for invasion of parathyroid tissue into adipose tissue (carcinoma); and (2) not to underestimate this abnormal gland as normal, especially on frozen section or if dealing with limited tissue. Pathologic, clinical, and serologic correlation is necessary!
Prognostically, these tumors behave as typical adenomas. There is no documented difference in pre-operative biochemistry. Importantly, confirmed by a recent series, there is no correlation between a patient’s body mass index (BMI) and the formation of a lipoadenoma.
References
- International Agency for Research on Cancer. Lloyd RV et al., eds: WHO classification of tumours of endocrine organs. 4th edition. 2017. International Agency for Research on Cancer: Lyon, France.
- Juhlin CC, et al. “Lipoadenoma of the Parathyroid Gland: Characterization of an Institutional Series Spanning 28 Years.” Endocr Pathol. 2020 Mar 19. doi: 10.1007/s12022-020-09616-3. [Epub ahead of print]
- Hyrcza MD, Sargın P, Mete O. “Parathyroid Lipoadenoma: a Clinicopathological Diagnosis and Possible Trap for the Unaware Pathologist.” Endocr Pathol. 2016 Mar;27(1):34-41. doi: 10.1007/s12022-015-9404-5.
Quiz Answers
Q1 = D. is comparable in terms of prognosis.
Q2 = B. False
Stephen M. Smith, MD
Assistant Professor, Division of Anatomic Pathology
Department of Laboratory Medicine & Pathobiology
The University of Toronto/University Health Network