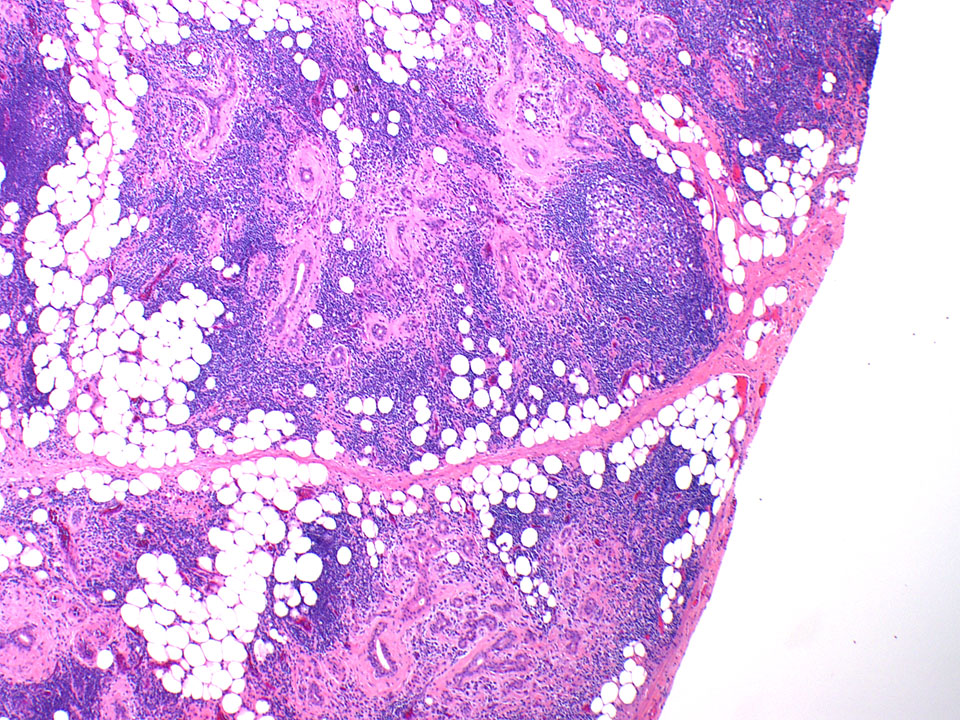
An 80-year-old female with a history of squamous cell carcinoma of the tongue that was treated by hemiglossectomy presented a year later with a tender right neck mass. A right radical neck dissection was performed, consisting predominantly of matted cervical lymph nodes with necrosis. In addition, Level IB contained a 3.0 cm well circumscribed, firm, tan-pink mass, shown below.
Q1. The histologic features are consistent with:
Q2. Which statement is TRUE about this disease?
Chronic sialadenitis
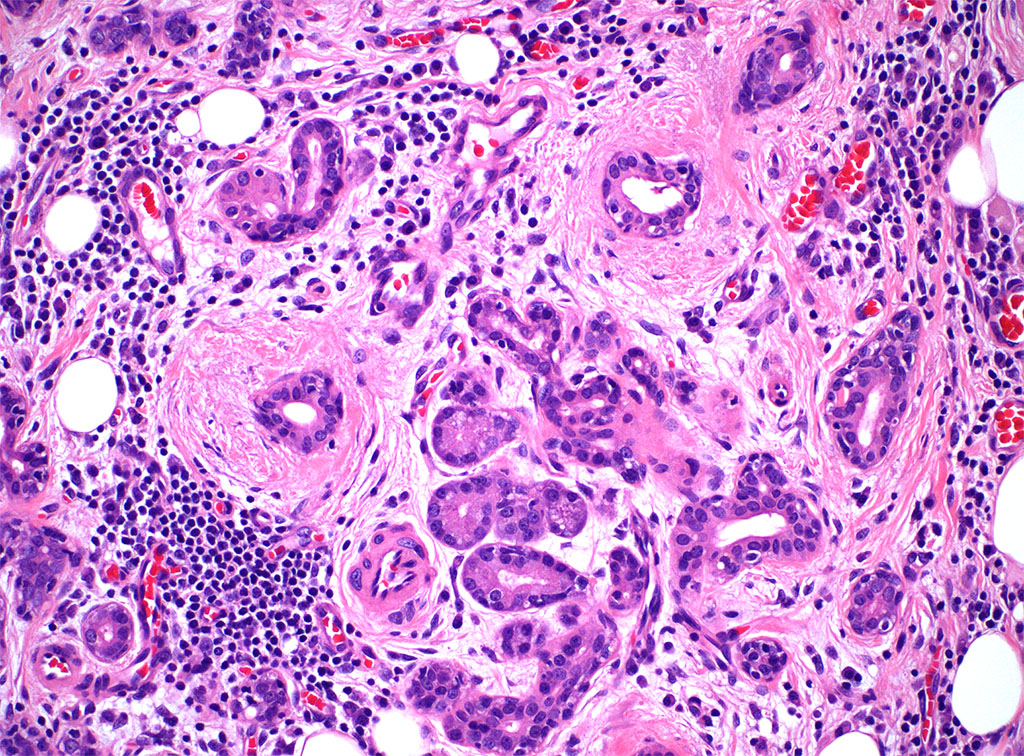
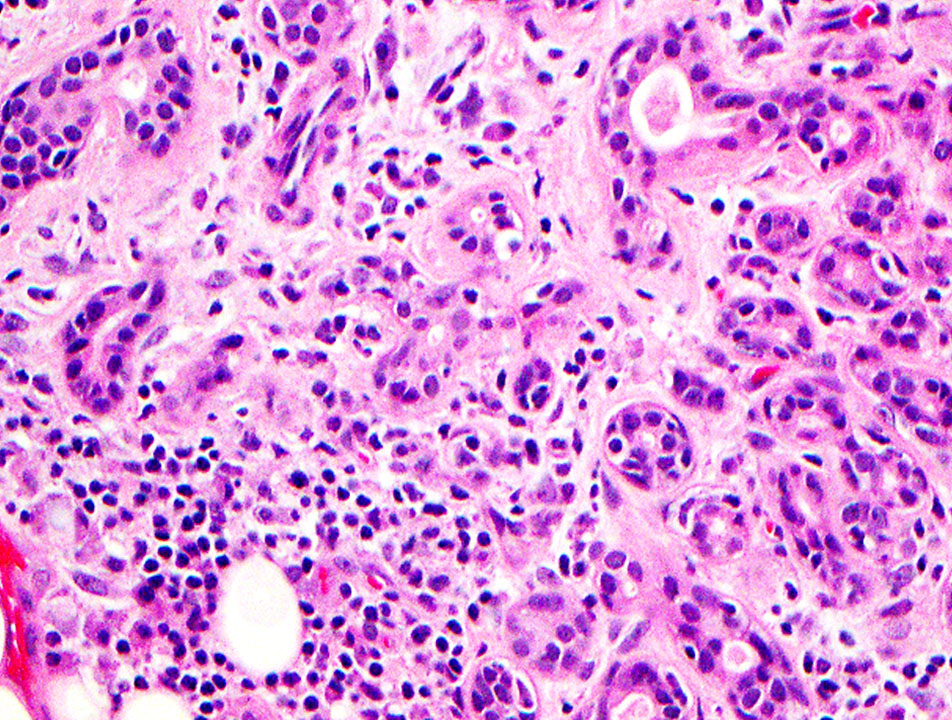
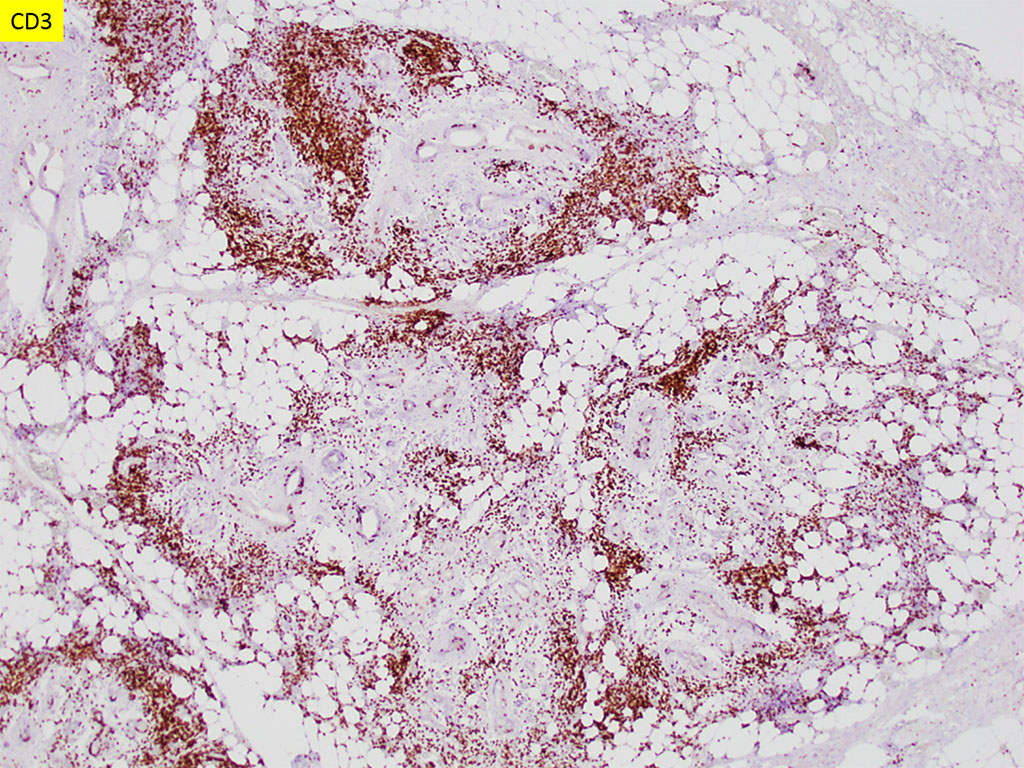
Chronic sialadenitis typically presents as pain and swelling related to mealtimes. Histologic features include varying degrees of lymphoplasmacytic inflammation with lymphoid aggregate formation, interlobular fibrosis, acinar atrophy, and ductal dilation. The lymphocytic cells are composed of a mixture of B and T cells.
There are many causes of chronic sialadenitis, but the most common is persistent or recurrent duct obstruction by calculi. Stricture or extrinsic compression by tumor can also impede salivary flow and result in similar changes. Sialadenitis may occur in patients treated by radiation therapy for head and neck cancers, with serous acini of the parotid being more sensitive than the mucous-cell-rich submandibular gland.
Systemic disorders (such as autoimmune conditions or Sjogren disease) histologically present with chronic inflammation, fibrosis, loss of acinar tissue, and characteristic ‘lymphoepithelial lesions’ (proliferations of ductal remnants which are infiltrated by lymphocytes). Clinically, there will be keratoconjunctivitis and/or xerostomia and the swelling is commonly bilateral. Correlation with serological findings of Ro(SS-A) and/or La(SS-B) autoantibodies, rheumatoid factor, and antinuclear antibody would also corroborate the diagnosis.
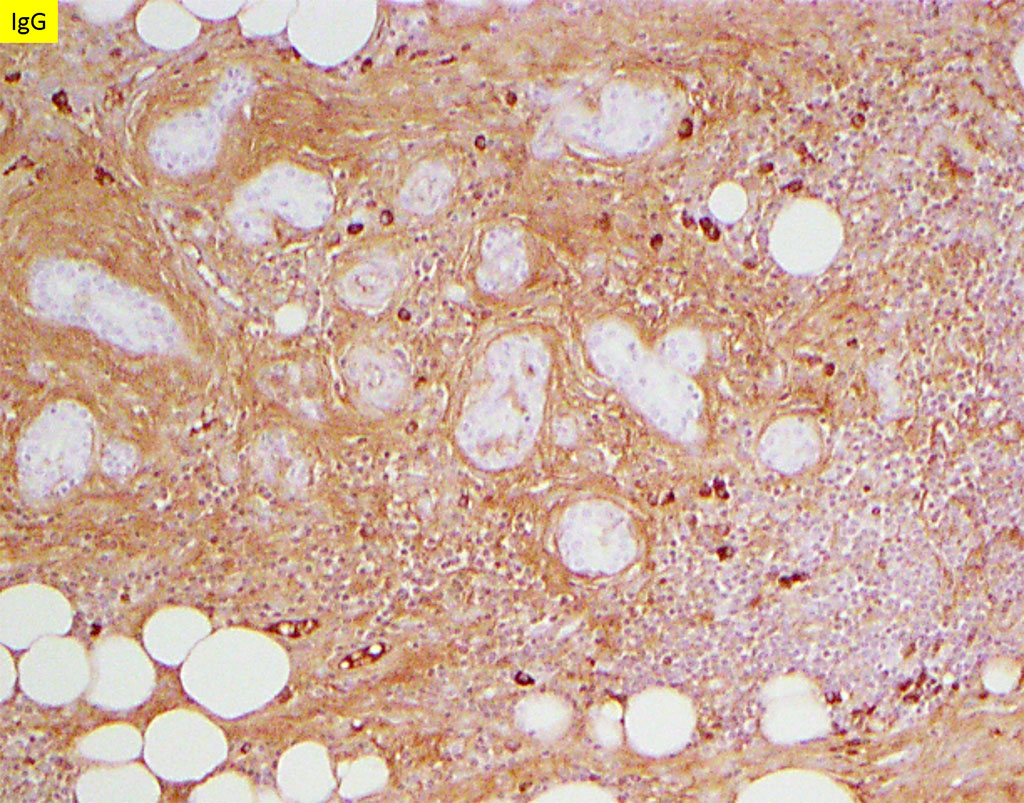
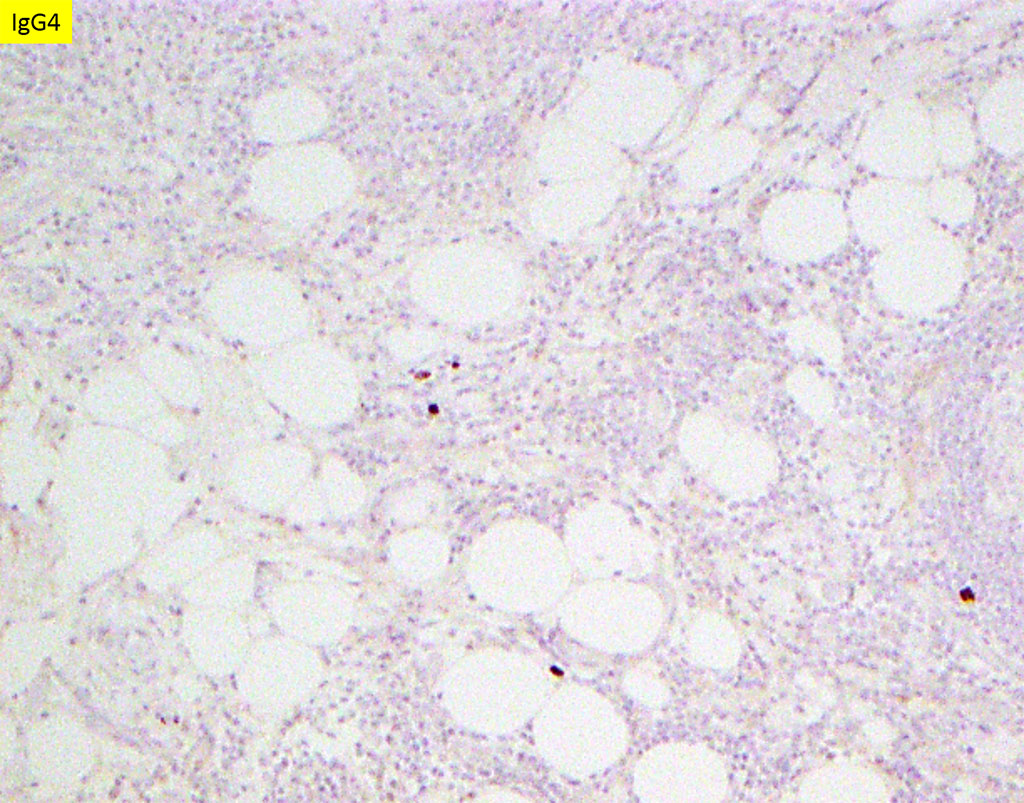
Immunoglobulin G4-related disease (IgG4-RD) is an immune-mediated fibroinflammatory condition that can affect the salivary glands. Distinctively, IgG4-related sialadenitis exhibits storiform fibrosis, obliterative phlebitis, and dense lymphoplasmacytic infiltrates with larger germinal center formation. In addition, it is characterized by markedly increased numbers of IgG4-positive plasma cells, compared to chronic sialadenitis or Sjogren syndrome. Typically, the ratio of IgG4:IgG positive plasma cells is >40% and serologic studies show IgG4 levels of >135 mg/dl in diagnostic cases.
Extranodal marginal zone B cell lymphoma may also be a diagnostic consideration. A lymphoproliferative disorder is suspected by a loss of lobular architecture with extension of atypical monoclonal B-lymphocytes beyond the capsule and into the adjacent tissues. The neoplastic cells are small to medium in size with relatively abundant pale cytoplasm that imparts a monocytoid appearance. These cells are CD19+, CD20+, CD79a+, CD3-, CD5-, CD10-, CD23-, and cyclin D1- and demonstrate light chain restriction. Further ancillary testing, such as cytogenetics and molecular studies, may also be used to evaluate for associated chromosomal translocations and/or genetic mutations.
It should be noted that fine needle aspiration is not useful in the diagnosis of chronic sialadenitis due to non-specific findings of the aspirate, which also tends to be paucicellular. In the present case, the patient did not have autoimmune disorders, radiation therapy, or sialolithiasis. The most significant finding was that of marked encasement of the carotid artery and nearby muscular branches supplying the submandibular gland by the squamous cell carcinoma. Given the unilateral presentation of the mass lesion, we include ischemia as a cause of chronic sialadenitis.
In conclusion, the constellation of lymphoplasmacytic inflammation, fibrosis, and acinar loss with sialoliths supports the diagnosis of chronic sialadenitis. Several other causes of chronic sialadenitis have been suggested, including ischemia, as presented in this case.
References
- Geyer JT, Ferry JA, Harris NL, et al. Chronic sclerosing sialadenitis (Küttner tumor) is an IgG4-associated disease. Am J Surg Pathol. 2010;34(2):202-210. doi:10.1097/PAS.0b013e3181c811ad
- Xu WL, Ling YC, Wang ZK, Deng F. Diagnostic performance of serum IgG4 level for IgG4-related disease: a meta-analysis. Sci Rep. 2016;6:32035. Published 2016 Aug 25. doi:10.1038/srep32035
- Geyer JT, Deshpande V. IgG4-associated sialadenitis. Curr Opin Rheumatol. 2011 Jan;23(1):95-101. doi: 10.1097/BOR.0b013e3283413011. PMID: 21124091.
- Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, Matsui S, Yoshino T, Nakamura S, Kawa S, Hamano H, Kamisawa T, Shimosegawa T, Shimatsu A, Nakamura S, Ito T, Notohara K, Sumida T, Tanaka Y, Mimori T, Chiba T, Mishima M, Hibi T, Tsubouchi H, Inui K, Ohara H. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012 Feb;22(1):21-30. doi: 10.1007/s10165-011-0571-z. Epub 2012 Jan 5. PMID: 22218969.
- Neville B, Damm D Allen C and Chi A. Oral and Maxillofacial Pathology ed.4. Elsevier, 2016.
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J (Eds): WHO Calssification of Tumours of Haematopoietic and Lymphoid Tissues (Revised 4th edition).IARC: Lyon 2017.
Quiz Answers
Q1 = D. Chronic sialadenitis
Q2 = C. It can result from compression by an adjacent tumor.