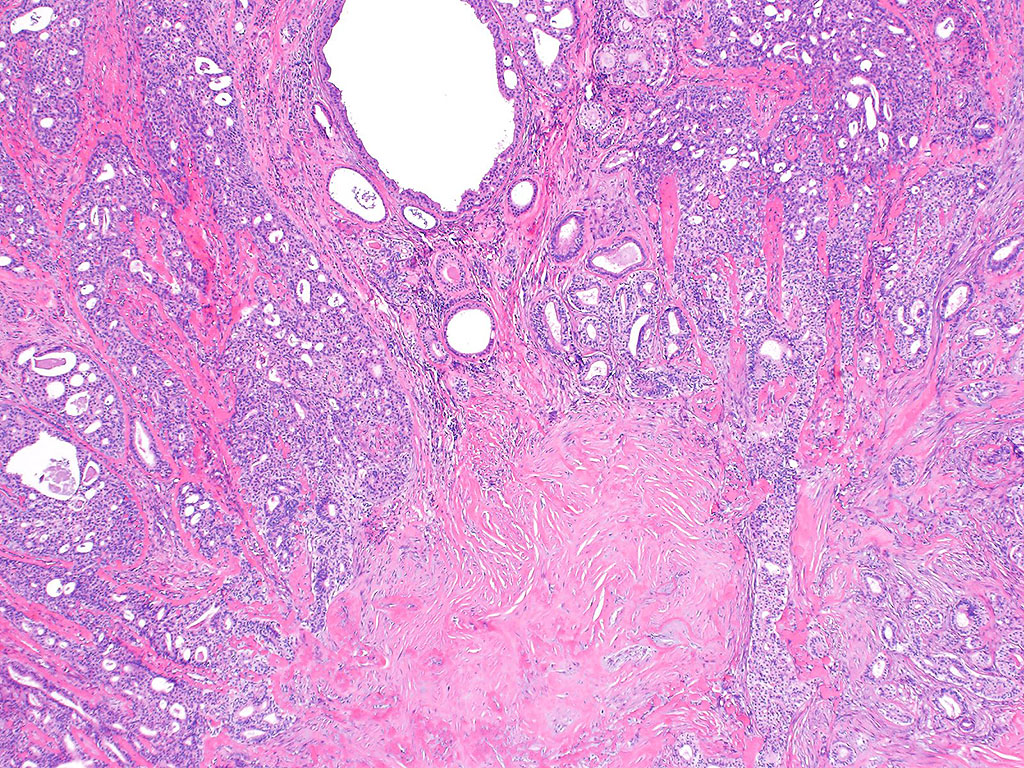
A boy presented to the pediatric otolaryngology clinic with a chief concern of mass in his left neck of several months’ duration. He was also experiencing mild intermittent pain. There was no lymphadenopathy. Pre-operative imaging studies identified an intraparotid nodule. A superficial parotidectomy was performed. H&E sections of the nodule are shown.
Q1. Which gene is most likely to harbor an alteration in this patient’s tumor?
Q2. This tumor type is associated with a considerable rate of recurrence.
Sclerosing polycystic adenoma / Sclerosing polycystic adenosis
Sclerosing polycystic adenoma/sclerosing polycystic adenosis is a rare benign lesion of salivary glands. It occurs over a wide age range from children to elderly with a male to female ratio of approximately 2:3. The most commonly involved salivary gland is parotid, followed by the submandibular gland. Most patients present with a singular, painless, slowly enlarging neck mass as an isolated condition without apparent association with other lesions.
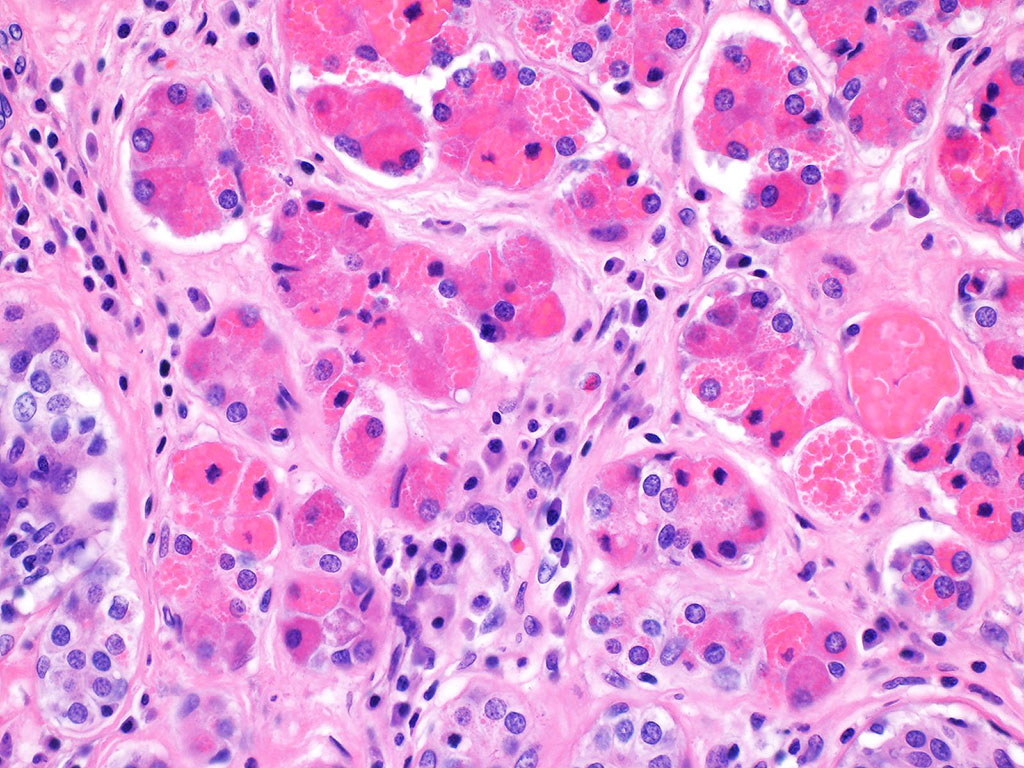
These lesions are often well-circumscribed with an absent or incomplete pseudocapsule and are surrounded by normal salivary gland tissue. The cut surface is typically solid with scattered tiny cystic spaces. Histologically, sclerosing polycystic adenoma/adenosis consists of a proliferation of cystic ductal structures and acinar cells surrounded by abundant hyalinized stromal collagen, exhibiting a characteristic lobular architecture. The acinar cells often contain abundant brightly eosinophilic cytoplasmic zymogen-like granules, a key histologic feature of this tumor type. Intraductal epithelial dysplastic proliferations may be seen, ranging from mild to severe dysplasia.
These lesions were initially considered to be a reactive or inflammatory process, and the term “sclerosing polycystic adenosis” was used. However, emerging evidence suggests a clonal process characterized by recurrent gene mutations in the PI3K pathway, with PTEN mutations identified in all analyzed cases. Therefore, the term “sclerosing polycystic adenoma” has been proposed to reflect the likely true neoplastic nature of this process.
Management of sclerosing polycystic adenoma is conservative surgical excision. Tumor recurrence is uncommon but remains significant.
References
- Smith BC, Ellis GL, Slater LJ, Foss RD. Sclerosing polycystic adenosis of major salivary glands. A clinicopathologic analysis of nine cases. Am J Surg Pathol. 1996;20(2):161-170.
- Gnepp DR, Wang LJ, Brandwein-Gensler M, Slootweg P, Gill M, Hille J. Sclerosing polycystic adenosis of the salivary gland: a report of 16 cases. Am J Surg Pathol. 2006;30(2):154-164.
- Skalova A, Gnepp DR, Simpson RH, et al. Clonal nature of sclerosing polycystic adenosis of salivary glands demonstrated by using the polymorphism of the human androgen receptor (HUMARA) locus as a marker. Am J Surg Pathol. 2006;30(8):939-944.
- Bishop JA, Gagan J, Baumhoer D, et al. Sclerosing Polycystic “Adenosis” of Salivary Glands: A Neoplasm Characterized by PI3K Pathway Alterations More Correctly Named Sclerosing Polycystic Adenoma. Head Neck Pathol. 2020;14(3):630-636.
Quiz Answers
Q1 = D. PTEN
Q2 = A. True