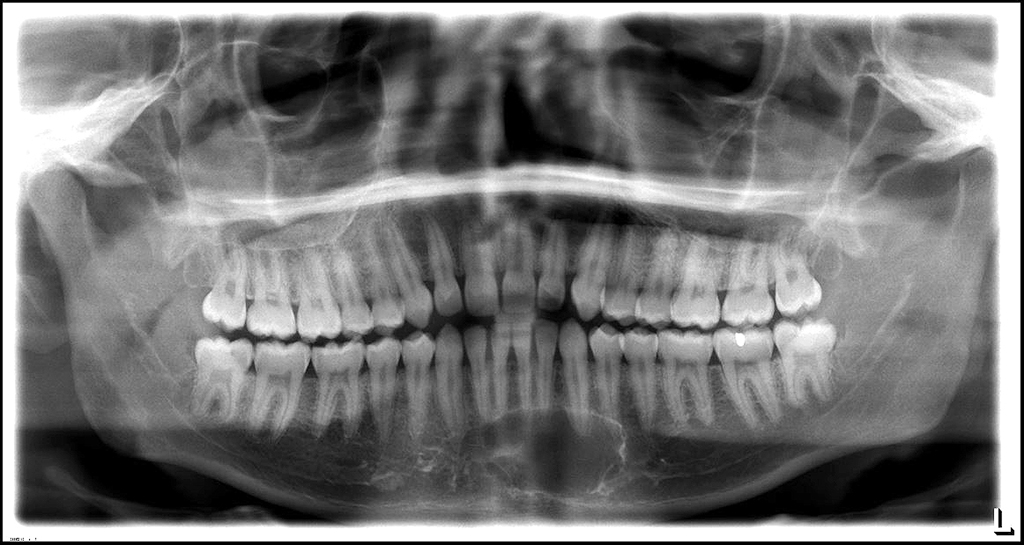
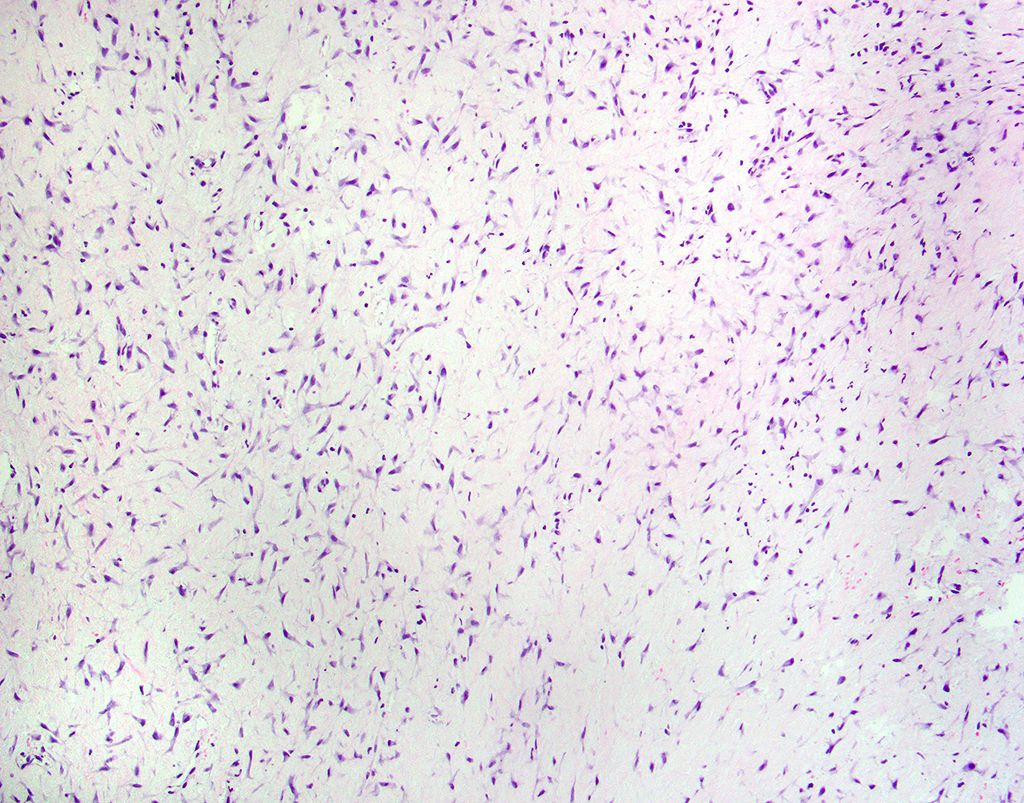
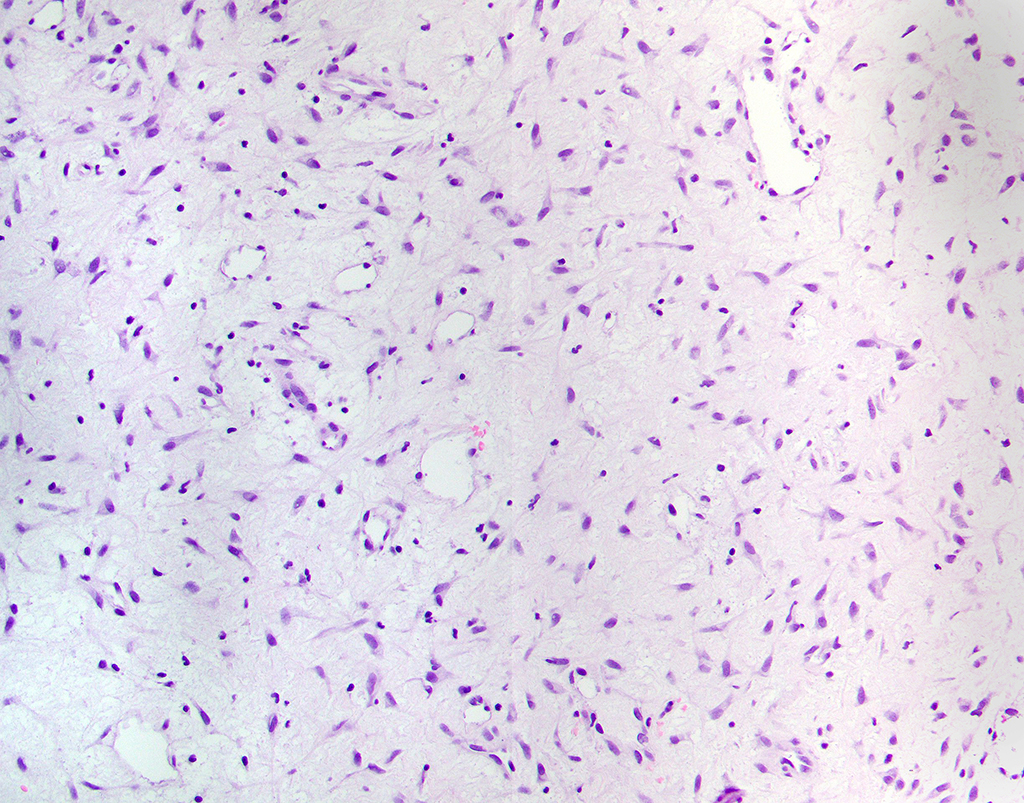
A 19-year-old male presented for initial dental examination upon entering the armed forces. His medical history was non-contributory, and he was asymptomatic. Panoramic radiographic examination (below) revealed a radiolucency of the anterior mandible. The lesion was vaguely multilocular with a corticated and smooth border and crossed the midline. Mild clinical expansion was noted. An incisional biopsy was performed, and the findings are represented in the photomicrographs below.
Q1. This lesion is most often found in which area of the jaws?
Q2. The radiographic features in this case are suggestive of malignancy.
Q3. This tumor does not have a known association with Carney complex.
Odontogenic Myxoma.
Odontogenic myxoma is a benign neoplasm derived from odontogenic ectomesenchyme. It is the third-most common odontogenic tumor, after odontoma and ameloblastoma. Patients are typically in their second or third decades of life at the time of diagnosis, but this tumor has been reported in patients of nearly all ages. Odontogenic myxomas are found exclusively in the gnathic bones. Two thirds of tumors are found in the mandible, with a predilection for the posterior regions. Myxomas of the maxilla tend to be destructive, obliterating the maxillary sinuses early in the disease process.
Clinically, patients may be asymptomatic or demonstrate painless swelling of the jaw. Odontogenic myxomas may cause marked expansion, and cortical perforation may occur. Radiographically, myxomas present as well-defined unilocular or multilocular radiolucencies. Some cases exhibit the classic radiologic feature: a soap-bubble appearance. Displacement and/or resorption of adjacent teeth occurs often. Cortication of the borders is seen on panoramic imaging, but myxomas are better visualized by computed tomography (CT) or magnetic resonance (MR) imaging, because they diffusely infiltrate the surrounding bone.
Intraoperatively, a glistening grey to white mass is encountered. Tumor consistency is variable, depending on the ratio of collagen to myxoid ground substance present.
Histologically, odontogenic myxomas look similar to the dental papilla of a developing tooth. A hypocellular proliferation of delicate spindled cells in a myxoid background is characteristic. The cells are stellate with long cytoplasmic processes, and are regularly dispersed. Occasional odontogenic epithelial rests are identified in about 5% of cases, but this feature is not required for diagnosis. The matrix that supports the lesional cells is a myxoid ground substance, accompanied by a variable amount of collagen. If the collagenous component is prominent, the term “myxofibroma” may be applied, although there is no demonstrated difference in biologic behavior.
Immunohistochemically, the lesional cells of odontogenic myxoma are diffusely reactive with vimentin and focally reactive with smooth muscle actin. The ground substance is reactive with Alcian blue, and further investigation has demonstrated that it is composed mostly of the mucopolysaccharide, hyaluronic acid.
The differential diagnoses that should be considered include low-grade fibromyxoid sarcoma, myxoid nerve sheath tumors, chondromyxoid fibroma, and other myxoid sarcomas. It is also important to note that dental pulp may look very much like a myxoma; so, clinical and radiographic correlation is essential. Odontogenic myxomas are not related to Carney complex, nor to other syndromes which include soft tissue myxomas. There is, however, an association between odontogenic myxomas and tuberous sclerosis, as well as Gorlin syndrome.
Due to the infiltrative margins of odontogenic myxomas, curettage is ineffective. These tumors necessitate resection with uninvolved margins. The recurrence rate for odontogenic myxomas is roughly 25%, and the risk of malignant transformation is nearly 0.
References
- El-Naggar AK, Chan JKC, Grandis JR, et al. WHO Classification of Head and Neck Tumors (4th edition). IARC: Lyon 2017.
- Martinez-Mata G, Mosqueda-Taylor A, Carlos-Bregni R, et al. (2008) Odontogenic myxoma: clinic-pathological, immunohistochemical and ultrastructural findings of a multicentric series. Oral Oncol. 44:601-7.
- Kim J, Ellis GL. (1993) Dental follicular tissue: misinterpretation as odontogenic tumors. J Oral Maxillofac Surg 51:762-7.
- Boffano P, Gallescio C, Barreca A, et al. (2011) Surgical treatment of odontogenic myxoma. J Craniofac Surg 22:982-7.
- Banasser AM, Bawazir MM, Islam MN, et al. (2020) Odontogenic myxoma: a 23-year retrospective series of 38 cases. Head and Neck Pathol https://doi.org/10.1007/s12105-020-01191-7.
Quiz Answers
Q1 = B. Posterior mandible
Q2 = B. False
Q3 = A. True
Anne C. McLean-Holden, DMD1; Brenda L. Nelson, DDS, MS2