A 65 year-old male with no significant past medical history presents with fatigue, difficulty swallowing, and voice changes for several months duration. CT scan showed an 8 cm left-sided neck mass. The patient underwent left hemithyroidectomy and parathyroidectomy. CT imaging, H&E sections, and immunostains of the mass are shown.
Q1. All of the following are characteristic features of this tumor, EXCEPT:
Q2. CDC73 mutation is the molecular driver in the pathogenesis of this tumor.
Parathyroid carcinoma with spindle cell differentiation (sarcomatoid carcinoma)
Parathyroid carcinoma is a rare neoplasm, accounting for <1% of all malignancies and has a female-to-male ratio of ~1:1. It can be sporadic or familial, with the latter seen in 10-15% of patients with hyperparathyroidism-jaw tumor syndrome (HPT-JT) or in the setting of familial isolated hyperparathyroidism (FIHP). Other etiologies include external radiation to the neck and prolonged chief cell hyperplasia in patients with renal failure and celiac disease.
Clinically, there is excess secretion of parathyroid hormone with calcium levels often >14 mg/dL. Laboratory workup in our patient prior to surgery revealed a calcium level of 14 and a parathyroid hormone level of 600. As a result, many patients show symptoms of fatigue, weakness, weight loss, nausea/vomiting, and polyuria. Unlike parathyroid adenoma, patients often have a palpable neck mass.
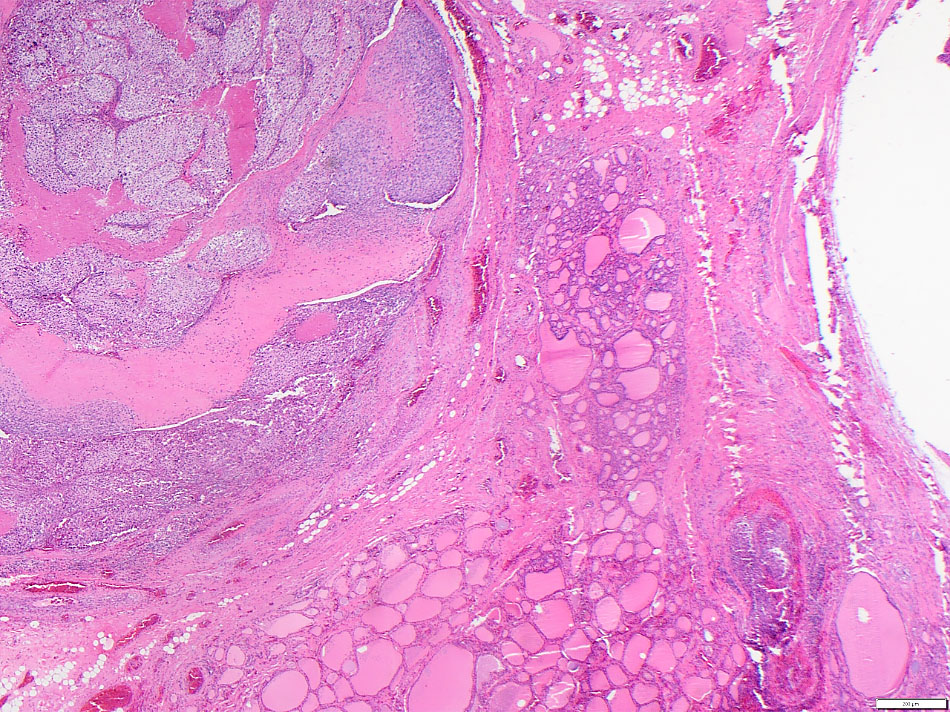
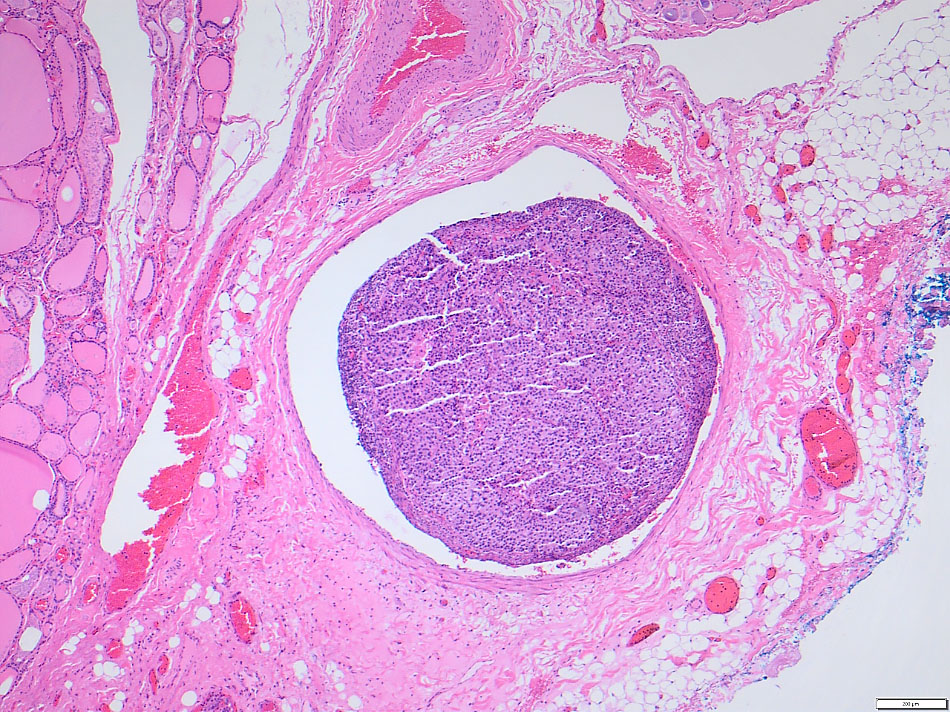
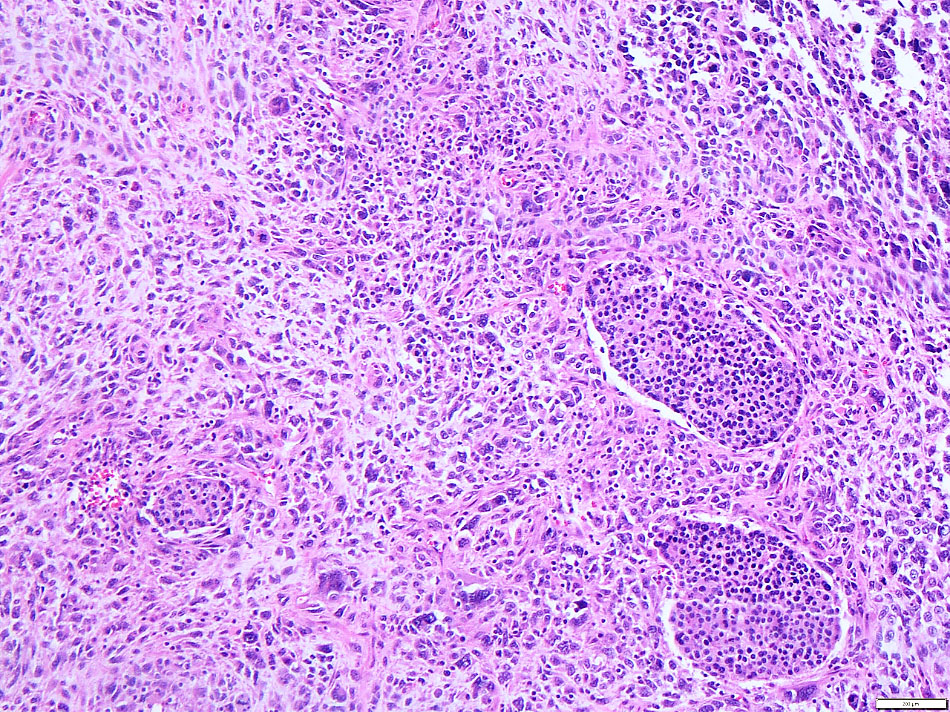
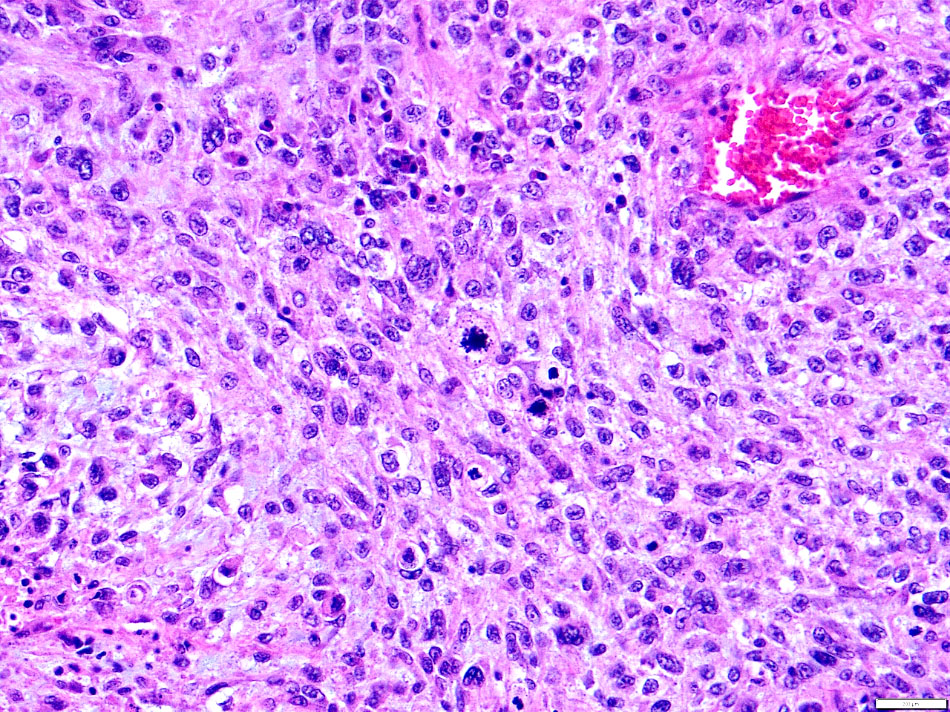
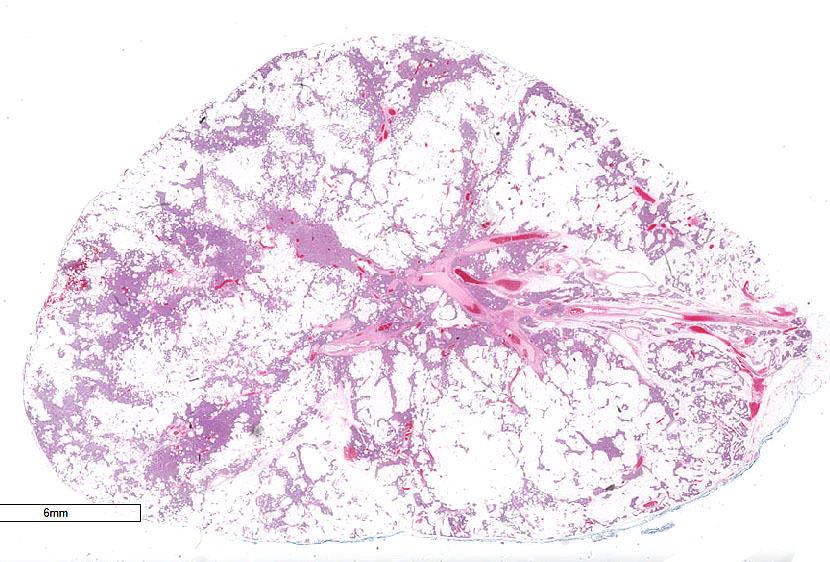
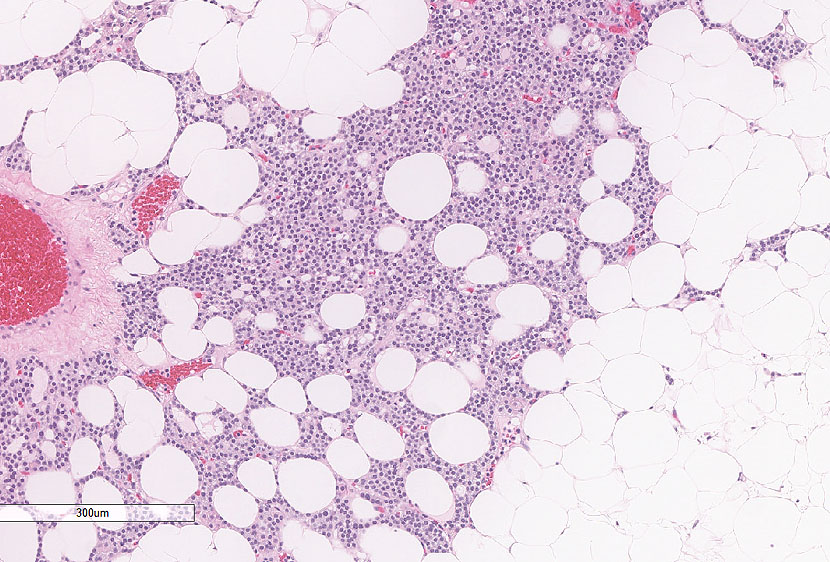
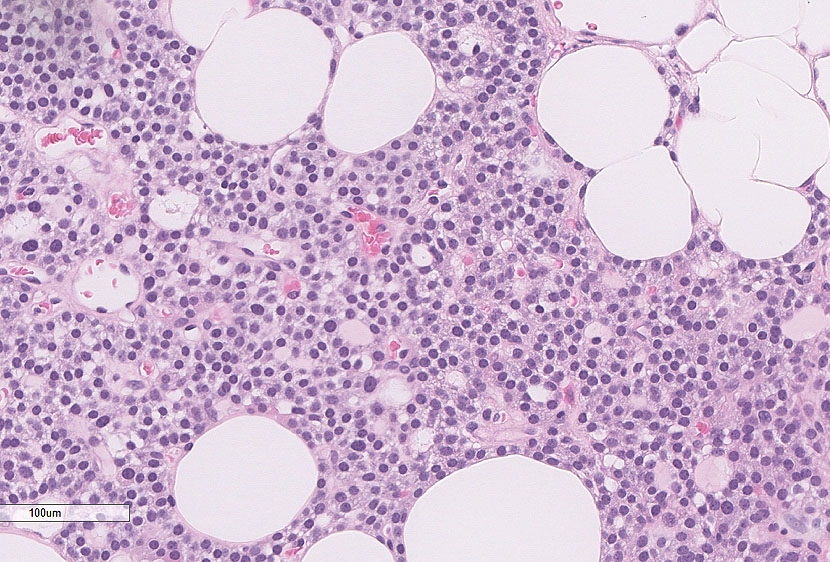
Grossly, tumors are often large, variably encapsulated, and ill-defined, involving the surrounding structures. In this patient, the tumor was grossly invading the thyroid and was also attached to the trachea and esophagus. On imaging, he also had multiple nodules in the lung, concerning for metastasis. Histologically, there is evidence of invasive growth involving the adjacent structures, vascular and/or perineural invasion. As in follicular thyroid carcinoma, vascular invasion should be in the surrounding soft tissue and not intratumoral. Tumor cells are often separated by broad fibrous bands. The triad of macronucleoli, >5 mitoses per 50 high-power fields, and necrosis is predictive of aggressive growth. Rarely, as in this case, the tumor cells can have sarcomatoid growth pattern, characterized by marked cytologic atypia and spindle cell morphology. To our knowledge, there are only ~ 5 cases reported in the English literature with this morphology. Among these patients, 3 developed lung metastases and died within 5-7 months of diagnosis.
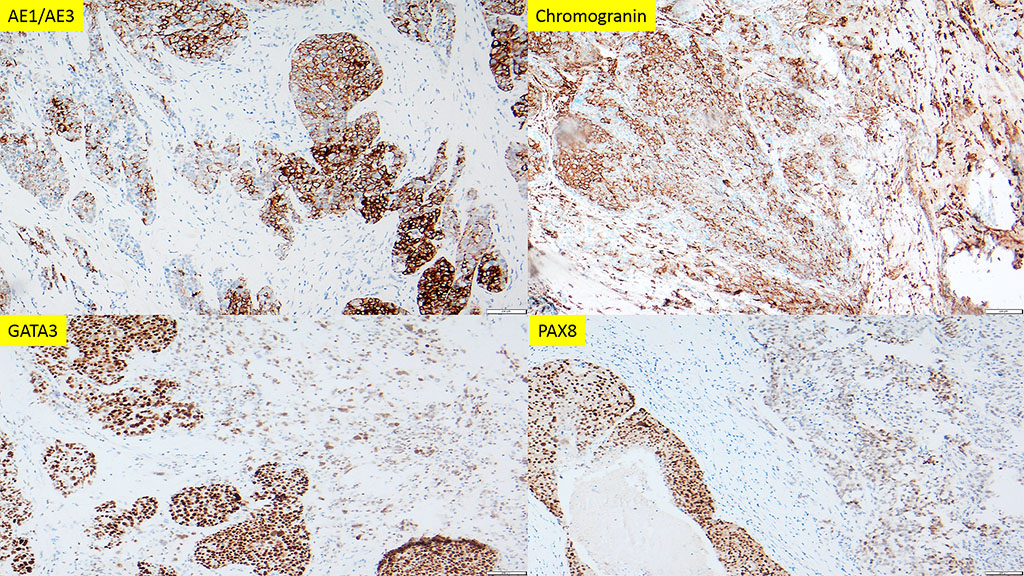
By immunohistochemistry, the tumor cells are positive for cytokeratins, PTH, GATA3, PAX8, synaptophysin, and chromogranin. Several studies, have shown inactivation of the tumor suppressor gene CDC73 as the major molecular driver in the pathogenesis of parathyroid carcinoma in both sporadic and familial forms.
Most parathyroid carcinomas recur locally, with spread to adjacent structures, such as the thyroid gland, strap muscles and recurrent laryngeal nerve. Older age, large tumor size, and male sex have been associated with worse overall survival. There is no generally accepted staging system for this tumor.
References
- Hu L, Xie X. Parathyroid carcinoma with sarcomatoid differentiation: a case report and literature review. Diagn Pathol. 2020 Dec 14;15(1):142. doi: 10.1186/s13000-020-01060-5. PMID: 33317559; PMCID: PMC7737283.
- Lloyd RV, Osamura RY, Kloppel G, Rosai J. WHO classification of Tumours of Endocrine Organs (4th edition). IARC: Lyon 2017.
- Harari A, Waring A, Fernandez-Ranvier G, Hwang J, Suh I, Mitmaker E, Shen W, Gosnell J, Duh QY, Clark O. Parathyroid carcinoma: a 43-year outcome and survival analysis. J Clin Endocrinol Metab. 2011 Dec;96(12):3679-86. doi: 10.1210/jc.2011-1571. Epub 2011 Sep 21. PMID: 21937626.
- Hu Y, Zhang X, Wang O, Bi Y, Xing X, Cui M, Wang M, Tao W, Liao Q, Zhao Y. The genomic profile of parathyroid carcinoma based on whole-genome sequencing. Int J Cancer. 2020 Nov 1;147(9):2446-2457. doi: 10.1002/ijc.33166. Epub 2020 Jul 24. PMID: 32574388.
Quiz Answers
Q1 = D. Rare recurrence after resection
Q2 = A. True